They’re small, fluffy, and kind of cute, but these mice represent a milestone in de-extinction efforts, according to their creators. The animals have undergone a series of genetic tweaks that give them features similar to those of woolly mammoths—and their creation may bring scientists a step closer to resurrecting the giant animals that roamed the tundra thousands of years ago.
“It’s a big deal,” says Beth Shapiro, chief science officer at Colossal Biosciences, the company behind the work. Scientists at Colossal have been working to “de-extinct” the woolly mammoth since the company was launched four years ago. Now she and her colleagues have shown they can create healthy animals that look the way the team wants them to look, she says.
“The Colossal woolly mouse marks a watershed moment in our de-extinction mission,” company cofounder Ben Lamm said in a statement. “This success brings us a step closer to our goal of bringing back the woolly mammoth.”
Colossal’s researchers say their ultimate goal is not to re-create a woolly mammoth wholesale. Instead, the team is aiming for what they call “functional de-extinction”—creating a mammoth-like elephant that can survive in something like the extinct animal’s habitat and potentially fulfill the role it played in that ecosystem. Shapiro and her colleagues hope that an “Arctic-adapted elephant” might make that ecosystem more resilient to climate change by helping to spread the seeds of plants, for example.
But other experts take a more skeptical view. Even if they succeed in creating woolly mammoths, or something close to them, we can’t be certain that the resulting animals will benefit the ecosystem, says Kevin Daly, a paleogeneticist at University College Dublin and Trinity College Dublin. “I think this is a very optimistic view of the potential ecological effects of mammoth reintroduction, even if everything goes to plan,” he says. “It would be hubristic to think we might have a complete grasp on what the introduction of a species such as the mammoth might do to an environment.”
Mice and mammoths
Woolly mammoth DNA has been retrieved from freeze-dried remains of animals that are tens of thousands of years old. Shapiro and her colleagues plan to eventually make changes to the genomes of modern-day elephants to make them more closely resemble those ancient mammoth genomes, in the hope that the resulting animals will look and behave like their ancient counterparts.
Before the team begins tinkering with elephants, Shapiro says, she wants to be confident that these kinds of edits work and are safe in mice. After all, Asian elephants, which are genetically related to woolly mammoths, are endangered. Elephants also have a gestation period of 22 months, which will make research slow and expensive. The gestation period of a mouse, on the other hand, is a mere 20 days, says Shapiro. “It makes [research] a lot faster.”
There are other benefits to starting in mice. Scientists have been closely studying the genetics of these rodents for decades. Shapiro and her colleagues were able to look up genes that have already been linked to wavy, long, and light-colored fur, as well as lipid metabolism. They made a shortlist of such genes that were also present in woolly mammoths but not in elephants.
The team identified 10 target genes in total. All were mouse genes but were thought to be linked to mammoth-like features. “We can’t just put a mammoth gene into a mouse,” says Shapiro. “There’s 200 million years of evolutionary divergence between them.”
Shapiro and her colleagues then carried out a set of experiments that used CRISPR and other gene-editing techniques to target these genes in groups of mice. In some cases, the team directly altered the genomes of mouse embryos before transferring them to surrogate mouse mothers. In other cases, they edited cells and injected the resulting edited cells into early-stage embryos before implanting them into other surrogates.
In total, 34 pups were born with varying numbers of gene edits, depending on which approach was taken. All of them appear to be healthy, says Shapiro. She and her colleagues will publish their work at the preprint server bioRxiv, and it has not yet been peer-reviewed.
COLOSSAL
“It’s an important proof of concept for … the reintroduction of extinct genetic variants in living [animal groups],” says Linus Girdland Flink, a specialist in ancient DNA at the University of Aberdeen, who is not involved in the project but says he supports the idea of de-extinction.
The mice are certainly woolly. But the team don’t yet know if they’d be able to survive in the cold, harsh climates that woolly mammoths lived in. Over the next year, Shapiro and her colleagues plan to investigate whether the gene edits “conferred anything other than cuteness,” she says. The team will feed the mice different diets and expose them to various temperatures in the lab to see how they respond.
Back from the brink
Representatives of Colossal have said that they plan to create a woolly mammoth by 2027 or 2028. At the moment, the team is considering 85 genes of interest. “We’re still working to compile the ultimate list,” says Shapiro. The resulting animal should have tusks, a big head, and strong neck muscles, she adds.
Given the animal’s long gestation period, reaching a 2028 deadline would mean implanting an edited embryo into an elephant surrogate in the next year or so. Shapiro says that the team is “on track” to meet this target but adds that “there’s 22 months of biology that’s really out of our control.”
That timeline is optimistic, to say the least. The target date has already been moved by a year, and the company had originally hoped to have resurrected the thylacine by 2025. Daly, who is not involved in the study, thinks the birth of a woolly mammoth is closer to a decade away.
In any case, if the project is eventually successful, the resulting animal won’t be 100% mammoth: it will be a new animal. And it is impossible to predict how it will behave and interact with its environment, says Daly.
“When you watch Jurassic Park, you see dinosaurs … as we imagine they would have been, and how they might have interacted with each other in the past,” he says. “In reality, biology is incredibly complicated.” An animal’s behavior is shaped by everything from the embryo’s environment and the microbes it encounters at birth to social interactions. “All of those things are going to be missing for a de-extinct animal,” says Daly.
It is also difficult to predict how we’ll respond to a woolly mammoth. “Maybe we’ll just treat them as [tourist attractions], and ruin any kind of ecological benefits that they might have,” says Daly. Colossal’s director of species conservation told MIT Technology Review in 2022 that the company might eventually sell tickets to see its de-extinct animals.
The team at Colossal is also working on projects to de-extinct the dodo as well as the thylacine. In addition, team members are interested in using biotech to help conservation of existing animals that are at risk of extinction. When a species dwindles, the genetic pool can shrink. This has been the fate of the pink pigeon, a genetic relative of the dodo that lives in Mauritius. The number of pink pigeons is thought to have shrunk to about 10 individuals twice in the last century.
A lack of genetic diversity can leave a species prone to disease. Shapiro and her colleagues are looking for more genetic diversity in DNA from museum specimens. They hope to be able to “edit diversity” back into the genome of the modern-day birds.
The Hawaiian honeycreeper is especially close to Shapiro’s heart. “The honeycreepers are in danger of becoming extinct because we [humans] introduced avian malaria into their habitat, and they don’t have a way to fight [it],” she says. “If we could come up with a way to help them to be resistant to avian malaria, then that will give them a chance at survival.”
Girdland Flink, of the University of Aberdeen, is more interested in pigs. Farmed pigs have also lost a lot of genetic diversity, he says. “The genetic ancestry of modern pigs looks nothing like the genetic ancestry of the earliest domesticated pigs,” he says. Pigs are vulnerable to plenty of viral strains and are considered to be “viral incubators.” Searching the genome of ancient pig remains for extinct—and potentially beneficial—genetic variants might provide us with ways to make today’s pigs more resilient to disease.
“The past is a resource that can be harnessed,” he says.
This article first appeared in The Checkup, MIT Technology Review’s weekly biotech newsletter. To receive it in your inbox every Thursday, and read articles like this first, sign up here.
This week I’ve been working on a story about a brain of glass. About five years ago, archaeologists found shiny black glass fragments inside the skull of a man who died in the Mount Vesuvius eruption of 79 CE. It seems they are pieces of brain, turned to glass.
Scientists have found ancient brains before—some are thought to be at least 10,000 years old. But this is the only time they’ve seen a brain turn to glass. They’ve even been able to spot neurons inside it.
The man’s remains were found at Herculaneum, an ancient city that was buried under meters of volcanic ash following the eruption. We don’t know if there are any other vitrified brains on the site. None have been found so far, but only about a quarter of the city has been excavated.
Some archaeologists want to continue excavating the site. But others argue that we need to protect it. Further digging will expose it to the elements, putting the artifacts and remains at risk of damage. You can only excavate a site once, so perhaps it’s worth waiting until we have the technology to do so in the least destructive way.
After all, there are some pretty recent horror stories of excavations involving angle grinders, and of ancient body parts ending up in garages. Future technologies might eventually make our current approaches look similarly barbaric.
The inescapable fact of fields like archaeology or paleontology is this: When you study ancient remains, you’ll probably end up damaging them in some way. Take, for example, DNA analysis. Scientists have made a huge amount of progress in this field. Today, geneticists can crack the genetic code of extinct animals and analyze DNA in soil samples to piece together the history of an environment.
But this kind of analysis essentially destroys the sample. To perform DNA analysis on human remains, scientists typically cut out a piece of bone and grind it up. They might use a tooth. But once it has been studied, that sample is gone for good.
Archaeological excavations have been performed for hundreds of years, and as recently as the 1950s, it was common for archaeologists to completely excavate a site they discovered. But those digs cause damage too.
Nowadays, when a site is discovered, archaeologists tend to focus on specific research questions they might want to answer, and excavate only enough to answer those questions, says Karl Harrison, a forensic archaeologist at the University of Exeter in the UK. “We will cross our fingers, excavate the minimal amount, and hope that the next generation of archaeologists will have new, better tools and finer abilities to work on stuff like this,” he says.
In general, scientists have also become more careful with human remains. Matteo Borrini, a forensic anthropologist at Liverpool John Moores University in the UK, curates his university’s collection of skeletal remains, which he says includes around 1,000 skeletons of medieval and Victorian Britons. The skeletons are extremely valuable for research, says Borrini, who himself has investigated the remains of one person who died from exposure to phosphorus in a match factory and another who was murdered.
When researchers ask to study the skeletons, Borrini will find out whether the research will somehow alter them. “If there is destructive sampling, we need to guarantee that the destruction will be minimal, and that there will be enough material [left] for further study,” he says. “Otherwise we don’t authorize the study.”
If only previous generations of archaeologists had taken a similar approach. Harrison told me the story of the discovery of “St Bees man,” a medieval man found in a lead coffin in Cumbria, UK, in 1981. The man, thought to have died in the 1300s, was found to be extraordinarily well preserved—his skin was intact, his organs were present, and he even still had his body hair.
Normally, archaeologists would dig up such ancient specimens with care, using tools made of natural substances like stone or brick, says Harrison. Not so for St Bees man. “His coffin was opened with an angle grinder,” says Harrison. The man’s body was removed and “stuck in a truck,” where he underwent a standard modern forensic postmortem, he adds.
“His thorax would have been opened up, his organs [removed and] weighed, [and] the top of his head would have been cut off,” says Harrison. Samples of the man’s organs “were kept in [the pathologist’s] garage for 40 years.”
If St Bees man were discovered today, the story would be completely different. The coffin itself would be recognized as a precious ancient artifact that should be handled with care, and the man’s remains would be scanned and imaged in the least destructive way possible, says Harrison.
Even Lindow man, who was discovered a mere three years later in nearby Manchester, got better treatment. His remains were found in a peat bog, and he is thought to have died over 2,000 years ago. Unlike poor St Bees man, he underwent careful scientific investigation, and his remains took pride of place in the British Museum. Harrison remembers going to see the exhibit when he was 10 years old.
Harrison says he’s dreaming of minimally destructive DNA technologies—tools that might help us understand the lives of long-dead people without damaging their remains. I’m looking forward to covering those in the future. (In the meantime, I’m personally dreaming of a trip to—respectfully and carefully—visit Herculaneum.)
Now read the rest of The Checkup
Read more from MIT Technology Review‘s archive
Some believe an “ancient-DNA revolution” is underway, as scientists use modern technologies to learn about human, animal, and environmental remains from the past. My colleague Antonio Regalado has the details in his recent feature. The piece was published in the latest edition of our magazine, which focuses on relationships.
Next-generation obesity drugs might be too effective. One trial participant lost 22% of her body weight in nine months. Another lost 30% of his weight in just eight months. (STAT)
A US court upheld the conviction of Elizabeth Holmes, the disgraced founder of the biotechnology company Theranos, who was sentenced to over 11 years for defrauding investors out of hundreds of millions of dollars. Her sentence has since been reduced by two years for good behavior. (The Guardian)
An unvaccinated child died of measles in Texas. The death is the first reported as a result of the outbreak that is spreading in Texas and New Mexico, and the first measles death reported in the US in a decade. Health and Human Services Secretary Robert F. Kennedy Jr. appears to be downplaying the outbreak. (NBC News)
A mysterious disease with Ebola-like symptoms has emerged in the Democratic Republic of Congo. Hundreds of people have been infected in the last five weeks, and more than 50 people have died. (Wired)
Towana Looney has been discharged from the hospital three months after receiving a gene-edited pig kidney. “I’m so grateful to be alive and thankful to have received this incredible gift,” she said. (NYU Langone)
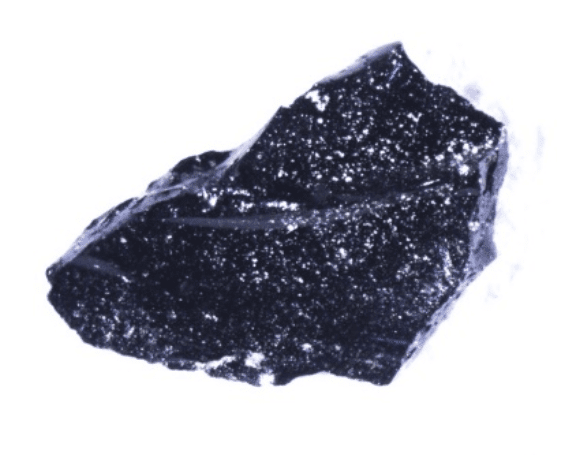
They look like small pieces of obsidian, smooth and shiny. But a set of small black fragments found inside the skull of a man who died in the eruption of Mount Vesuvius in Southern Italy, in the year 79 CE, are thought to be pieces of his brain—turned to glass.
The discovery, reported in 2020, was exciting because a human brain had never been found in this state. Now, scientists studying his remains believe they’ve found out more details about how the glass fragments were formed: The man was exposed to temperatures of over 500 °C, followed by rapid cooling. These conditions also allowed for the preservation of tiny structures and cells inside his brain.
“It’s an extraordinary finding,” says Matteo Borrini, a forensic anthropologist at Liverpool John Moores University in the UK, who was not involved in the research. “It tells us how [brain] preservation can work … extreme conditions can produce extreme results.”
Glittering remains
The Roman city of Herculaneum has been covered in ash for many hundreds of years. Excavations over the last few centuries have revealed amazing discoveries of preserved bodies, buildings, furniture, artworks, and even food. They’ve helped archaeologists piece together a picture of what life was like for people living in ancient Rome. But they are still yielding surprises.
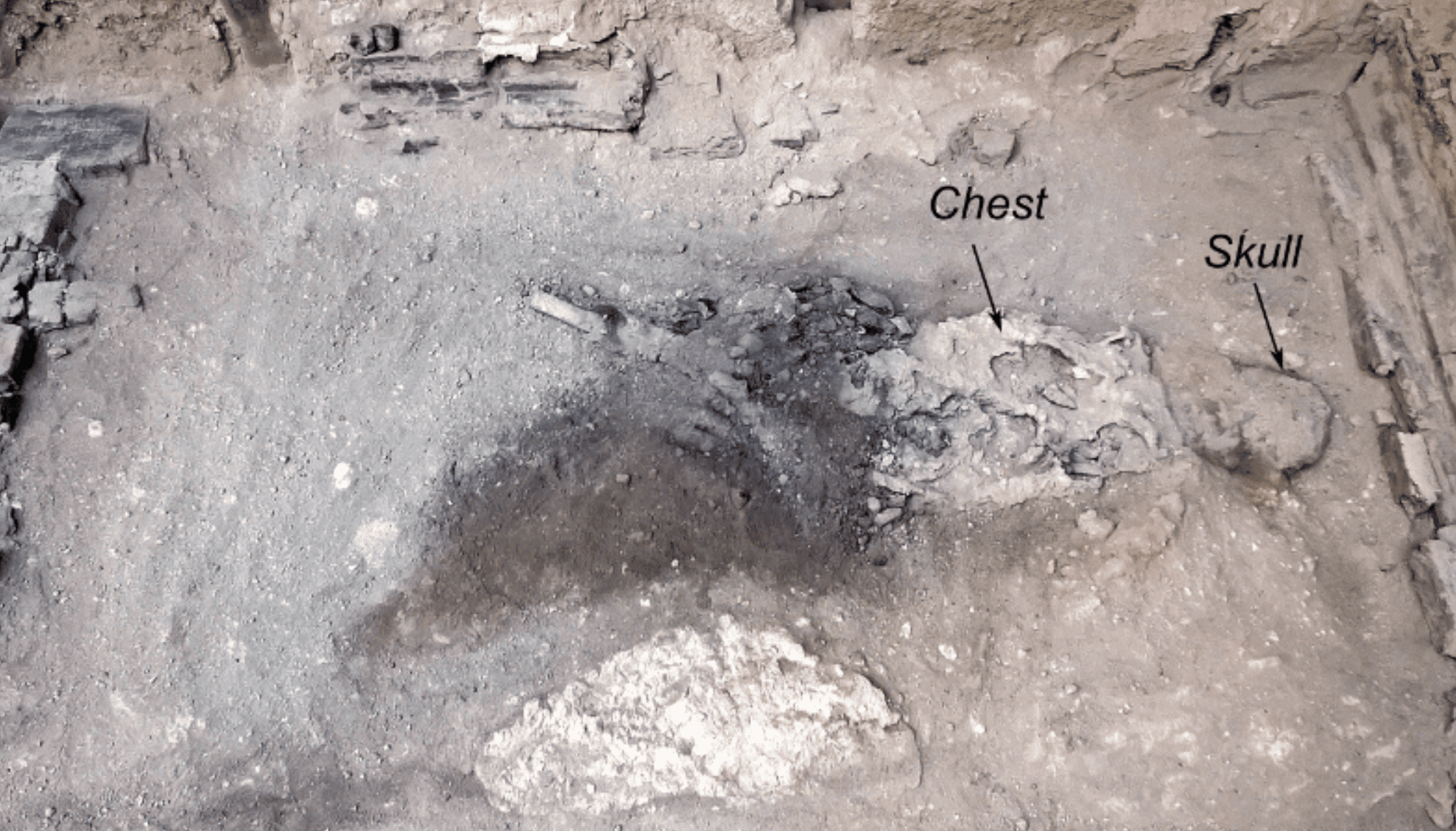
Around five years ago, Pier Paolo Petrone, a forensic archaeologist at the University of Naples Federico II, was studying remains first excavated in the 1960s of what is believed to be a 20-year-old man. The man was found inside a building thought to have been a place of worship. Archaeologists believe he may have been guarding the building. He was found lying face down on a wooden bed.
The carbonized remains of the deceased individual in their bed in Herculaneum.
GUIDO GIORDANO ET AL./SCIENTIFIC REPORTS
Petrone was documenting the man’s charred bones under a lamp when he noticed something unusual. “I suddenly saw small glassy remains glittering in the volcanic ash that filled the skull,” he tells MIT Technology Review via email. “It had a black appearance and shiny surfaces quite similar to obsidian.” But, he adds, “unlike obsidian, the glassy remains were extremely brittle and easy to crumble.”
An analysis of the proteins in the sample suggested that the glassy remains were preserved brain tissue. And when Petrone and his colleagues studied bits of the material with microscopes, they were even able to see neurons. “I [was] very excited because I understood that [the preserved brain] was something very unique, never seen before in any other archaeological or forensic context,” he says.
The next question was how the man’s brain turned to glass in the first place, says Guido Giordano, a volcanologist at Roma Tre University in Rome, who was also involved in the research. To find out, he and his colleagues subjected tiny pieces of the glass brain fragments—measuring millimeters wide—to extreme temperatures in the lab. The goal was to identify its “glass transition state”—the temperature at which the material changed from brittle to soft.
GUIDO GIORDANO ET AL./SCIENTIFIC REPORTS
These experiments suggest that the material is a glass, and that it formed when the temperature dropped from above 510 °C to room temperature, says Giordano. “The heating stage would not have been long. Otherwise the material would have been … cooked, and disappeared,” he says. This, he adds, is probably what happened to the brains of the other people whose remains were found at Herculaneum, which were not preserved.
The short periods of extremely high temperature might have resulted from super-hot volcanic gases and a few centimeters’ worth of ash, which enveloped the city shortly after the eruption and settled. Denser pyroclastic flows from the volcano would have hit the building hours later, possibly after the brain had a chance to rapidly cool down.
“The ash clouds can easily be 500 or 600 degrees … [but] they may quickly pass and quickly vanish,” says Giordano, who, along with his colleagues, published the results in the journal Scientific Reports on Thursday. “That would provide the fast cooling that is required to produce the glass.”
A unique case
No one knows for sure why this young man’s brain was the only one to form glass fragments. It might have been because he was sheltered inside the building, says Giordano. It is thought that most of Herculaneum’s other residents flocked to the city’s shores, hoping to be rescued.
It’s also not clear why the man was found lying face down on a bed. “We don’t know what he was doing,” says Giordano. He might not have been guarding the building at all, says Karl Harrison, a forensic archaeologist at the University of Exeter in the UK. “In a fire, people will end up in rooms they don’t know, because they’re running through smoke,” he says. The conditions may have been similar during the volcanic eruption. “People end up in funny places,” he adds.
Either way, it’s a unique finding. Archaeologists have unearthed ancient human brains before—over 4,400 have been discovered since the mid-17th century. But these samples tend to have been preserved through drying, freezing, or a process called saponification, in which the brains “effectively turn to soap,” says Harrison. He was involved in work on a site in Turkey at which an 8,000-year-old brain was found. That brain appears to have “carbonized” and turned charcoal-like, he says.
Some of the glassy brain fragments remain at the site in Herculaneum, but others are being kept at universities, where scientists plan to continue research on them. Petrone wants to further study the proteins in the samples to learn more about what’s in them.
Holding the fragments feels “quite amazing,” says Giordano. “A few times I stop and think: ‘I’m actually holding a bit of a brain of a human,’” he says. “It can be touching.”
This article first appeared in The Checkup, MIT Technology Review’s weekly biotech newsletter. To receive it in your inbox every Thursday, and read articles like this first, sign up here.
Yesterday marks a month since the inauguration of Donald Trump as the 47th US president. And what a month it has been. The Trump administration wasted no time in delivering a slew of executive orders, memos, and work notices to federal employees.
Making IVF more affordable and accessible should give people more options when it comes to family planning and reproductive freedom more generally. But the move comes after a barrage of actions by the new administration that are hitting reproductive care hard for people around the world. On January 20, his first day in office, Trump ordered a “90-day pause in United States foreign development assistance” for such programs to be assessed. By January 24, a “stop work” memo issued by the State Department brought US-funded aid programs around the world to a halt.
Recent estimates suggest that more than 8,000 women will die from complications related to pregnancy and childbirth over the next 90 days if the funding is not reinstated.
On January 24 Trump also reinstated the global gag rule—a policy that requires nongovernmental organizations receiving US health funding to agree that they will not offer abortion counseling and care. This move alone immediately stripped organizations of the funding they need to perform their work. MSI Reproductive Choices, which offers support for reproductive health care in 36 countries, lost $14 million as a result, says Anna Mackay, who manages donor-funded programs at the organization. “Over 2 million women and girls would have received contraceptive services with that money,” she says.
The US Agency for International Development (USAID) had a 2025 budget of $42.8 billion to spend on foreign assistance, which covers everything from humanitarian aid and sanitation to programs promoting gender equality and economic growth in countries around the world. But the “stop work” memo froze that funding for 90 days.
The impacts were felt immediately and are still rippling out. Clinical trials were halted. Jobs were lost. Health programs were shut down.
“I think this is going to have a devastating impact on the global health architecture,” says Thoai Ngo at Columbia University’s Mailman School of Public Health. “USAID is the major foreign funder for global health … I’m afraid that there isn’t [another government] that can fill the gap.”
Reproductive health care is likely to lose out as affected governments and health organizations try to reorganize their resources, says Ngo: “In times of crisis … women and girls tend to be deprioritized in terms of access to health and social services.”
Without information on and access to a range of contraceptive options, unintended pregnancies result. These have the potential to limit the freedoms of people who become pregnant. And they can have far-reaching economic impacts, since access to contraception can improve education rates and career outcomes.
And the health consequences can be devastating. Unintended pregnancies are more likely to be ended with abortions—potentially unsafe ones. Maternal death rates are high in regions that lack adequate resources. A maternal death occurred every two minutes in 2020.
“It’s difficult to overstate how catastrophic this freeze has been over the last several weeks,” says Amy Friedrich-Karnik, director of federal policy at the Guttmacher Institute, a research and policy organization focused on global sexual and reproductive health and rights. “Every single day that the freeze is in place, there are 130,000 women who are being denied contraceptive care,” she says.
The Guttmacher Institute estimates that should USAID funding be frozen for the full 90 days, around 11.7 million women and girls would lose access to contraceptive care, and 4.2 million of them would experience unintended pregnancies. Of those, “8,340 will die from complications during pregnancy and childbirth,” says Friedrich-Karnik.
“By denying people access to contraception, not only are you denying them tools for their bodily autonomy—you are really risking their lives,” she says. “Thousands more women will die down the road.”
“USAID plays such a central role in supporting these life-saving programs,” says Ngo. “The picture is bleak.”
Even online sources of information on contraceptives are being affected by the funding freeze. Ben Bellows is a chief business officer at Nivi, a digital health company that develops chatbots to deliver health information to people via WhatsApp. “Two million users have used the bot,” he says.
He and his team have been working on a project to deliver information on contraceptive options and family planning to women in India, and they have been looking to incorporate AI into their bot. The project was funded by a company that, in turn, is funded by USAID. Like the funding, the work is “frozen,” says Bellows.
“We’ve slowed [hiring] and we’ve slowed some of the tech development because of the freeze [on USAID],” he says. “It’s bad [for] the individuals, it’s bad [for] the companies that are trying to operate in these markets, and it’s bad [for] public health outcomes.”
Reproductive health and freedoms are also likely to be affected by the Trump administration’s cuts to federal agencies. The National Institutes of Health and the Centers for Disease Control and Prevention have been in the administration’s crosshairs, as has the Food and Drug Administration.
After all, the FDA regulates drugs and medical devices in the US, including contraceptives. The CDC collects and shares important data on sexual and reproductive health. And the NIH supports vital research on reproductive health and contraception.
The CDC also funds health programs in low-income countries like Ethiopia. Following Trump’s executive order, the country’s ministry of health terminated the contracts of more than 5,000 health workers whose salaries were supported by the CDC as well as USAID.
“That’s midwives and nurses working in rural health posts,” says Mackay. “We’re turning up to support these staff and provide them with sexual reproductive health training and make sure they’ve got the contraceptives, and there’s just no one at the facility.”
So, yes, it is great news if the Trump administration can find a way to make IVF more accessible. But, as Mackay points out, “it’s increasing reproductive choice in one direction.”
My colleague Rhiannon Williams reported on the immediate aftermath of the decision that reversed Roe v. Wade.
Fertility rates are falling around the world, in almost every country. IVF is great, but it won’t save us from a looming fertility crisis. Gender equality and family-friendly policies are much more likely to be effective.
Decades of increasingly successful IVF treatments have caused millions of embryos to be stored in cryopreservation tanks around the world. In some cases, they can’t be donated, used, or destroyed and appear to be stuck in limbo “forever.”
Ever come across the term “women of childbearing age”? The insidious idea that women’s bodies are, above all else, vessels for growing children has plenty of negative consequences for us all. But it has also set back scientific research and health policy.
The US Food and Drug Administration assesses the efficacy and toxicity of experimental medicines before they are approved. It should also consider their “financial toxicity,” given that medical bills can fall on the shoulders of patients themselves, argue a group of US doctors. (The New England Journal of Medicine)
Robert F. Kennedy Jr., the new US secretary of health and human services, has vowed to investigate the country’s childhood vaccination schedule. During his confirmation hearing a couple of weeks ago, he promised not to change the schedule. (Associated Press)
Some scientists have been altering their published work without telling anyone. Such “stealth corrections” threaten scientific integrity, say a group of researchers from Europe and the US. (Learned Publishing)
The US Department of Agriculture said it accidentally fired several people who were working on the federal response to the bird flu outbreak. Apparently the agency is now trying to hire them back. (NBC News)
Could your next pet be a glowing rabbit? This startup is using CRISPR to “level up” pets. Their goal is to eventually create a real-life unicorn. (Wired)
Eske Willerslev was on a tour of Montreal’s Redpath Museum, a Victorian-era natural history collection of 700,000 objects, many displayed in wood and glass cabinets. The collection—“very, very eclectic,” a curator explained—reflects the taste in souvenirs of 19th-century travelers and geology buffs. A visitor can see a leg bone from an extinct Steller’s sea cow, a suit of samurai armor, a stuffed cougar, and two human mummies.
Willerslev, a well-known specialist in obtaining DNA from old bones and objects, saw potential biological samples throughout this hodgepodge of artifacts. Glancing at a small Egyptian cooking pot, he asked the tour leader, “Do you ever find any grain in these?” After studying a dinosaur skeleton that proved to be a cast, not actual bone, he said: “Too bad. There can be proteins on the teeth.”
“I am always thinking, ‘Is there something interesting to take DNA from?’” he said, glancing at the curators. “But they don’t like it, because …” Willerslev, who until recently traveled with a small power saw, made a back-and-forth slicing motion with his hand.
Willerslev was visiting Montreal to receive a science prize from the World Cultural Council—one previously given to the string theorist Edward Witten and the astrophysicist Margaret Burbidge, for her work on quasars. Willerslev won it for “numerous breakthroughs in evolutionary genetics.” These include recovering the first more or less complete genome of an ancient man, in 2010, and setting a record for the oldest genetic material ever retrieved: 2.4-million-year-old genes from a frozen mound in Greenland, which revealed that the Arctic desert was once a forest, complete with poplar, birch, and roaming mastodons.
These findings are only part of a wave of discoveries from what’s being called an “ancient-DNA revolution,” in which the same high-speed equipment used to study the DNA of living things is being turned on specimens from the past. At the Globe Institute, part of the University of Copenhagen, where Willerslev works, there’s a freezer full of human molars and ear bones cut from skeletons previously unearthed by archaeologists. Another holds sediment cores drilled from lake bottoms, in which his group is finding traces of entire ecosystems that no longer exist.
“We’re literally walking on DNA, both from the present and from the past.”
Eske Willerslev
Thanks to a few well-funded labs like the one in Copenhagen, the gene time machine has never been so busy. There are genetic maps of saber-toothed cats, cave bears, and thousands of ancient humans, including Vikings, Polynesian navigators, and numerous Neanderthals. The total number of ancient humans studied is more than 10,000 and rising fast, according to a December 2024 tally that appeared in Nature. The sources of DNA are increasing too. Researchers managed to retrieve an Ice Age woman’s genome from a carved reindeer tooth, whose surface had absorbed her DNA. Others are digging at cave floors and coming up with records of people and animals that lived there.
“We’re literally walking on DNA, both from the present and from the past,” Willerslev says.
Eske Willerslev leads one of a handful of laboratories pioneering the extraction and sequencing of ancient DNA from humans, animals, and the environment. His group’s main competition is at Harvard University and at the Max Planck Institute for Evolutionary Anthropology in Leipzig, Germany.
JONAS PRYNER ANDERSEN
The old genes have already revealed remarkable stories of human migrations around the globe. But researchers are hoping ancient DNA will be more than a telescope on the past—they hope it will have concrete practical use in the present. Some have already started mining the DNA of our ancestors for clues to the origin of modern diseases, like diabetes and autoimmune conditions. Others aspire to use the old genetic data to modify organisms that exist today.
At Willerslev’s center, for example, a grant of 500 million kroner ($69 million) from the foundation that owns the Danish drug company Novo Nordisk is underwriting a project whose aims include incorporating DNA variation from plants that lived in ancient climates into the genomes of food crops like barley, wheat, and rice. The plan is to redesign crops and even entire ecosystems to resist rising temperatures or unpredictable weather, and it is already underway—last year, barley shoots bearing genetic information from plants that lived in Greenland 2 million years ago, when temperatures there were far higher than today, started springing up in experimental greenhouses.
Willerslev, who started out looking for genetic material in ice cores, is leaning into this possibility as the next frontier of ancient-DNA research, a way to turn it from historical curiosity to potential planet-saver. If nothing is done to help food crops adapt to climate change, “people will starve,” he says. “But if we go back into the past in different climate regimes around the world, then we should be able to find genetic adaptations that are useful. It’s nature’s own response to a climate event. And can we get that? Yes, I believe we can.”
Shreds and traces
In 1993, just a day before the release of the blockbuster Steven Spielberg film Jurassic Park, scientists claimed in a paper that they had extracted DNA from a 120-million-year-old weevil preserved in amber. The discovery seemed to bring the film’s premise of a cloned T. rex closer to reality. “Sooner or later,” a scientist said at the time, “we’re going to find amber containing some biting insect that filled its stomach with blood from a dinosaur.”
But those results turned out to be false—likely the result of contamination by modern DNA. The problem is that modern DNA is much more abundant than what’s left in an old tooth or sample of dirt. That’s because the genetic molecule is constantly chomped on by microbes and broken up by water and radiation. Over time, the fragments get smaller and smaller, until most are so short that no one can tell whether they belonged to a person or a saber-toothed cat.
“Imagine an ancient genome as a big old book, and that all the pages have been torn out, put through a shredder, and tossed into the air to be lost with the wind. Only a few shreds of paper remain. Even worse, they are mixed with shreds of paper from other books, old and new,” says Elizabeth Jones, a science historian. Her 2022 book, Ancient DNA: The Making of a Celebrity Science, details researchers’ overwhelming fear of contamination—both literal, from modern DNA, and of the more figurative sort that can occur when scientists are so tempted by the prospect of fame and being first that they risk spinning sparse data into far-fetched stories.
“When I entered the field, my supervisor said this is a very, very dodgy path to take,” says Willerslev.
But the problem of mixed-up and fragmented old genes was largely solved beginning in 2005, when US companies first introduced ultra-fast next-generation machinery for analyzing genomes. These machines, meant for medical research, required short fragments for fast performance. And ancient-DNA researchers found they could use them to brute-force their way through even poorly preserved samples. Almost immediately, they started recovering large parts of the genomes of cave bears and woolly mammoths.
Ancient humans were not far behind. Willerslev, who was not yet famous, didn’t have access to human bones, and definitely not the bones of Neanderthals (the best ones had been corralled by the scientist Svante Pääbo, who was already analyzing them with next-gen sequencers in Germany). But Willerslev did learn about a six-inch-long tuft of hair collected from a 4,000-year-old midden, or trash heap, on Greenland’s coast. The hair had been stored in a plastic bag in Denmark’s National Museum for years. When he asked about it, curators told him they thought it was human but couldn’t be sure.
“Well, I mean, do you know any other animal in Greenland with straight black hair?” he says. “Not really, right?”
The hair turned out to contain well-preserved DNA, and in 2010, Willerslev published a paper in Nature describing the genome of “an extinct Paleo-Eskimo.” It was the first more or less complete human genome from the deep past. What it showed was a man with type A+ blood, probably brown eyes and thick dark hair, and—most tellingly—no descendants. His DNA code had unique patterns not found in the Inuit who occupy Greenland today.
“Give the archaeologists credit … because they have the hypothesis. But we can nail it and say, ‘Yes, this is what happened.’”
Lasse Vinner
The hair had come from a site once occupied by a group called the Saqqaq, who first reached Greenland around 4,500 years ago. Archaeologists already knew that the Saqqaq’s particular style of making bird darts and spears had vanished suddenly, but perhaps that was because they’d merged with another group or moved away. Now the man’s genome, with specific features pointing to a genetic dead end, suggested they really had died out, very possibly because extreme isolation, and inbreeding, had left them vulnerable. Maybe there was a bad year when the migrating reindeer did not appear.
“Give the archaeologists credit … because they have the hypothesis. But we can nail it and say, ‘Yes, this is what happened,’” says Lasse Vinner, who oversees daily operations at the Copenhagen ancient-DNA lab. “We’ve substantiated or falsified a number of archaeological hypotheses.”
In November, Vinner, zipped into head-to-toe white coveralls, led a tour through the Copenhagen labs, located in the basement of the city’s Natural History Museum. Samples are processed there in a series of cleanrooms under positive air pressure. In one, the floors were still wet with bleach—just one of the elaborate measures taken to prevent modern DNA from getting in, whether from a researcher’s shoes or from floating pollen. It’s partly because of the costly technologies, cleanrooms, and analytical expertise required for the work that research on ancient human DNA is dominated by a few powerful labs—in Copenhagen, at Harvard University, and in Leipzig, Germany—that engage in fierce competition for valuable samples and discoveries. A 2019 New York Times Magazine investigation described the field as an “oligopoly,” rife with perverse incentives and a smash-and-grab culture—in other words, artifact chasing straight out of Raiders of the Lost Ark.
To get his share, Willerslev has relied on his growing celebrity, projecting the image of a modern-day explorer who is always ready to trade his tweeds for muck boots and venture to some frozen landscape or Native American cave. Add to that a tale of redemption. Willerslev often recounts his struggles in school and as a would-be mink hunter in Siberia (“I’m not only a bad student—I’m also a tremendously bad trapper,” he says) before his luck changed once he found science.
This narrative has made him a favorite on television programs like Nova and secured lavish funding from Danish corporations. His first autobiography was titled From Fur Hunter to Professor. A more recent one is called simply It’s a Fucking Adventure.
Peering into the past
The scramble for old bones has produced a parade of headlines about the peopling of the planet, and especially of western Eurasia—from Iceland to Tehran, roughly. That’s where most ancient DNA samples originate, thanks to colder weather, centuries of archaeology, and active research programs. At the National Museum in Copenhagen, some skeletons on display to the public have missing teeth—teeth that ended up in the Globe Institute’s ancient-DNA lab as part of a project to analyze 5,000 sets of remains from Eurasia, touted as the largest single trove of old genomes yet.
What ancient DNA uncovered in Europe is a broad-brush story of three population waves of modern humans. First to come out of Africa were hunter-gatherers who dispersed around the continent, followed by farmers who spread out of Anatolia starting 11,000 years ago. That wave saw the establishment of agriculture and ceramics and brought new stone tools. Last came a sweeping incursion of people (and genes) from the plains of modern Ukraine and Russia—animal herders known as the Yamnaya, who surged into Western Europe spreading the roots of the Indo-European languages now spoken from Dublin to Bombay.
Mixed history
The DNA in ancient human skeletons reveals prehistoric migrations.
The genetic background of Europeans was shaped by three major migrations starting about 45,000 years ago. First came hunter-gatherers. Next came farmers from Anatolia, bringing crops and new ways of living. Lastly, mobile herders called the Yamnaya spread from the steppes of modern Russia and Ukraine. The DNA in ancient skeletons holds a record of these dramatic population changes.
Adapted from “100 ancient genomes show repeated population turnovers in Neolithic Denmark,” Nature, January 10, 2024, and “Tracing the peopling of the world through genomics,” Nature, January 18, 2017
Archaeologists had already pieced together an outline of this history through material culture, examining shifts in pottery styles and burial methods, the switch from stone axes to metal ones. Some attributed those changes to cultural transmission of knowledge rather than population movements, a view encapsulated in the phrase “pots, not people.” However, ancient DNA showed that much of the change was, in fact, the result of large-scale migration, not all of which looks peaceful. Indeed, in Denmark, the hunter-gatherer DNA signature all but vanishes within just two generations after the arrival of farmers during the late Stone Age. To Willerslev, the rapid population replacement “looks like some kind of genocide, to be honest.” It’s a guess, of course, but how else to explain the “limited genetic contribution” to subsequent generations of the blue-eyed, dark-haired locals who’d fished and hunted around Denmark’s islands for nearly 5,000 years? Certainly, the bodies in Copenhagen’s museums suggest violence—some have head injuries, and one still has arrows in it.
In other cases, it’s obvious that populations met and mixed; the average ethnic European today shares some genetic contribution from all three founding groups—hunter, farmer, and herder—and a little bit from Neanderthals, too.“We had the idea that people stay put, and if things change, it’s because people learned to do something new, through movements of ideas,” says Willerslev. “Ancient DNA showed that is not the case—that the transitions from hunter-gatherers to farming, from bronze to iron, from iron to Viking, [are] actually due to people coming and going, mixing up and bringing new knowledge.” It means the world that we observe today, with Poles in Poland and Greeks in Greece, “is very, very young.”
With an increasing number of old bodies giving up their DNA secrets, researchers have started to search for evidence of genetic adaptation that has occurred in humans since the last ice age (which ended about 12,000 years ago), a period that the Copenhagen group noted, in a January 2024 report, “involved some of the most dramatic changes in diet, health, and social organization experienced during recent human evolution.”
Every human gene typically comes in a few different possible versions, and by studying old bodies, it’s possible to see which of these versions became more common or less so with time—potentially an indicator that they’re “under selection,” meaning they influenced the odds that a person stayed alive to reproduce. These pressures are often closely tied to the environment. One clear signal that pops out of ancient European genes is a trend toward lighter skin—which makes it easier to produce vitamin D in the face of diminished sunlight and a diet based on grains.
DNA from ancient human skeletons could help us understand the origins of modern diseases, like multiple sclerosis.
MIKAL SCHLOSSER/UNIVERSITY OF COPENHAGEN
New technology and changing lifestyles—like agriculture and living in proximity to herd animals (and their diseases)—were also potent forces. Last fall, when Harvard University scientists scanned DNA from skeletons, they said they’d detected “rampant” evidence of evolutionary action. The shifts appeared especially in immune system genes and in a definite trend toward less body fat, the genetic markers of which they found had decreased significantly “over ten millennia.” That finding, they said, was consistent with the “thrifty gene” hypothesis, a feast-or-famine theory developed in the 1960s, which states that before the development of farming, people needed to store up more food energy, but doing so became less of an advantage as food became more abundant.
Many of the same genes that put people at risk for multiple sclerosis today almost certainly had some benefit in the past.
Such discoveries could start to explain some modern disease mysteries, such as why multiple sclerosis is unusually common in Nordic countries, a pattern that has perplexed doctors.
The condition seems to be a “latitudinal disease,” becoming more prevalent the farther north you go; theories have pointed to factors including the relative lack of sunlight. In January of last year, the Copenhagen team, along with colleagues, claimed that ancient DNA had solved the riddle, saying the increased risk could be explained in part by the very high amount of Yamnaya ancestry among people in Sweden, Norway, and Denmark.
When they looked at modern people, they found that mutations known to increase the risk of multiple sclerosis were far more likely to occur in stretches of DNA people had inherited from these Yamnaya ancestors than in parts of their genomes originating elsewhere.
There’s a twist to the story: Many of the same genes that put people at risk for multiple sclerosis today almost certainly had some benefit in the past. In fact, there’s a clear signal these gene versions were once strongly favored and on the increase. Will Barrie, a postdoc at Cambridge University who collaborated on the research, says the benefit could have been related to germs and infections that these pastoralists were getting from animals. But if modern people don’t face the same exposures, their immune system might still try to box at shadows, resulting in autoimmune disease. That aligns with evidence that children who aren’t exposed to enough pathogens may be more likely to develop allergies and other problems later in life.
“I think the whole sort of lesson of this work is, like, we are living with immune systems that we have inherited from our past,” says Barrie. “And we’ve plunged it into a completely new, modern environment, which is often, you know, sanitary.”
Telling stories about human evolution often involves substantial guesswork—findings are frequently reversed. But the researchers in Copenhagen say they will be trying to more systematically scan the past for health clues. In addition to the DNA of ancient peoples, they’re adding genetic information on what pathogens these people were infected with (germs based on DNA, like plague bacteria, can also get picked up by the sequencers), as well as environmental data, such as average temperatures at points in the past, or the amount of tree cover, which can give an idea of how much animal herding was going on. The resulting “panels”—of people, pathogens, and environments—could help scientists reach stronger conclusions about cause and effect.
Some see in this research the promise of a new kind of “evolutionary medicine”—drugs tailored to your ancestry. However, the research is not far enough along to propose a solution for multiple sclerosis.
For now, it’s just interesting. Barrie says several multiple sclerosis patients have written him and said they were comforted to think their affliction had an explanation. “We know that [the genetic variants] were helpful in the past. They’re there for a reason, a good reason—they really did help your ancestors survive,” he says. “I hope that’s helpful to people in some sense.”
Bringing things back
In Jurassic Park, which was the highest-grossing movie of all time until Titanic came out in 1997, scientists don’t just get hold of old DNA. They also use it to bring dinosaurs back to life, a development that leads to action-packed and deadly consequences.
The idea seemed like fantasy when the film debuted. But Jurassic Park presaged current ambitions to bring past genes into the present. Some of these efforts are small in scale. In 2021, for instance, researchers added a Neanderthal gene to human cells and turned those into brain organoids, which they reported were smaller and lumpier than expected. Others are aiming for living animals. Texas-based Colossal Biosciences, which calls itself the “first de-extinction company,” says it will be trying to use a combination of gene editing, cloning, and artificial wombs to re-create extinct species such as mammoths and the Tasmanian tiger, or thylacine.
Colossal recently recruited a well-known paleogenomics expert, Beth Shapiro, to be its chief scientist. In 2022, Shapiro, previously an advisor to the company, said that she had sequenced the genome of an extinct dodo bird from a skull kept in a museum. “The past, by its nature, is different from anything that exists today,” says Shapiro, explaining that Colossal is “reaching into the past to discover evolutionary innovations that we might use to help species and ecosystems thrive today and into the future.”
The idea of bringing extinct animals back to life seemed like fantasy when Jurassic Park debuted. But the film presaged current ambitions to bring past genes into the present.
It’s not yet clear how realistic the company’s plan to reintroduce missing species and restore nature’s balance really is, although the public would likely buy tickets to see even a poor copy of an extinct animal. Some similar practical questions surround the large grant Willerslev won last year from the philanthropic foundation of Novo Nordisk, whose anti-obesity drugs have turned it into Denmark’s most valuable company.
The project’s concept is to read the blueprints of long-gone ecosystems and look for genetic information that might help major food crops succeed in shorter or hotter growing seasons. Willerslev says he’s concerned that climate change will be unpredictable—it’s hard to say if it will be too wet in any particular area or too dry. But the past could offer a data bank of plausible solutions, which he thinks needs to be prepared now.
The prototype project is already underway using unusual mutations in plant DNA found in the 2-million-year-old dirt samples from Greenland. Some of these have been introduced into modern barley plants by the Carlsberg Group, a brewer that is among the world’s largest beer companies and operates an extensive crop lab in Copenhagen.
Eske Willerslev collects samples in the Canadian Arctic during a summer 2024 field trip. DNA preserved in soil could help determine how megafauna, like the woolly mammoth, went extinct.
RYAN WILKES/UNIVERSITY OF COPENHAGEN
One gene being studied is for a blue-light receptor, a protein that helps plants decide when to flower—a trait also of interest to modern breeders. Two and a half million years ago, the world was warm, and parts of Greenland particularly so—more than 10 °C hotter than today. That is why vegetation could grow there. But Greenland hasn’t moved, so the plants must have also been specially adapted to the stress of a months-long dusk followed by weeks of 24-hour sunlight. Willerslev says barley plants with the mutation are already being grown under different artificial light conditions, to see the effects.
“Our hypothesis is that you could use ancient DNA to identify new traits and as a blueprint for modern crop breeding,” says Birgitte Skadhauge, who leads the Carlsberg Research Laboratory. The immediate question is whether barley can grow in the high north—say, in Greenland or upper Norway, something that could be important on a warming planet. The research is considered exploratory and separate from Carlsberg’s usual commercial efforts to discover useful traits that cut costs—of interest since it brews 10 billion liters of beer a year, or enough to fill the Empire State Building nine times.
Scientists often try hit-or-miss strategies to change plant traits. But Skadhauge says plants from unusual environments, like a warm Greenland during the Pleistocene era, will have incorporated the DNA changes that are important already. “Nature, you know, actually adapted the plants,” she says. “It already picked the mutation that was useful to it. And if nature has adapted to climate change over so many thousands of years, why not reuse some of that genetic information?”
Many of the lake cores being tapped by the Copenhagen researchers cover more recent times, only 3,000 to 10,000 years ago. But the researchers can also use those to search for ideas—say, by tracing the genetic changes humans imposed on barley as they bred it to become one of humanity’s “founder crops.” Among the earliest changes people chose were those leading to “naked” seeds, since seeds with a sticky husk, while good for making beer, tend to be less edible. Skadhauge says the team may be able to reconstruct barley’s domestication, step by step.
There isn’t much precedent for causing genetic information to time-travel forward. To avoid any Jurassic Park–type mishaps, Willerslev says, he’s building a substantial ethics team “for dealing with questions about what does it mean if you’re introducing ancient traits into the world.” The team will have to think about the possibility that those plants could outcompete today’s varieties, or that the benefits would be unevenly distributed—helping northern countries, for example, and not those closer to the equator.
Willerslev says his lab’s evolution away from human bones toward much older DNA is intentional. He strongly hints that the team has already beat its own record for the oldest genes, going back even more than 2.4 million years. And as the first to look further back in time, he’s certain to make big discoveries—and more headlines. “It’s a blue ocean,” he says—one that no one has ever seen.
A new adventure, he says, is practically guaranteed.
This article first appeared in The Checkup, MIT Technology Review’s weekly biotech newsletter. To receive it in your inbox every Thursday, and read articles like this first, sign up here.
Over the past couple of weeks, I’ve been speaking to people who have lost their voices. Both Joyce Esser, who lives in the UK, and Jules Rodriguez, who lives in Miami, Florida, have forms of motor neuron disease—a class of progressive disorders that result in the gradual loss of the ability to move and control muscles.
It’s a crushing diagnosis for everyone involved. Jules’s wife, Maria, told me that once it was official, she and Jules left the doctor’s office gripping each other in floods of tears. Their lives were turned upside down. Four and a half years later, Jules cannot move his limbs, and a tracheostomy has left him unable to speak.
“To say this diagnosis has been devastating is an understatement,” says Joyce, who has bulbar MND—she can still move her limbs but struggles to speak and swallow. “Losing my voice has been a massive deal for me because it’s such a big part of who I am.”
AI is bringing back those lost voices. Both Jules and Joyce have fed an AI tool built by ElevenLabs recordings of their old voices to re-create them. Today, they can “speak” in their old voices by typing sentences into devices, selecting letters by hand or eye gaze. It’s been a remarkable and extremely emotional experience for them—both thought they’d lost their voices for good.
But speaking through a device has limitations. It’s slow, and it doesn’t sound completely natural. And, strangely, users might be limited in what they’re allowed to say.
Joyce doesn’t use her voice clone all that often. She finds it impractical for everyday conversations. But she does like to hear her old voice and will use it on occasion. One such occasion was when she was waiting for her husband, Paul, to get ready to go out.
Joyce typed a message for her voice clone to read out: “Come on, Hunnie, get your arse in gear!!” She then added: “I’d better get my knickers on too!!!”
“The next day I got a warning from ElevenLabs that I was using inappropriate language and not to do it again!!!” Joyce told me via email (we communicated with a combination of email, speech, text-to-voice tools, and a writing board). She wasn’t sure what had been inappropriate, exactly. It’s not as though she’d used any especially vile language—just, as she puts it, “normal British banter between a couple getting ready to go out.”
Joyce assumed that one of the words she’d used had been automatically flagged up by “the prudish American computer,” and that once someone from the ElevenLabs team had assessed the warning, it would be dismissed.
“Well, apparently not, because the next day a human banned me!!!!” says Joyce. She says she felt mortified. “I’d just got my voice back and now they’d taken it away from me … and only two days after I’d done a presentation to my local MND group telling them how amazing ElevenLabs were.”
Joyce contacted ElevenLabs, who apologized and reinstated her account. But it’s still not clear why she was banned in the first place. When I first asked Sophia Noel, a company representative, about the incident, she directed me to the company’s prohibited use policy.
There are rules against threatening child safety, engaging in illegal behavior, providing medical advice, impersonating others, interfering with elections, and more. But there’s nothing specifically about inappropriate language. I asked Noel about this, and she said that Joyce’s remark was most likely interpreted as a threat.
ElevenLabs’ terms of use state that the company does not have any obligation to screen, edit, or monitor content but add that it may “terminate or suspend” access to its services when content is “reasonably likely, in our sole determination, to violate applicable law or [the user] Terms.” ElevenLabs has a moderation tool that “screens content to ensure it aligns with our Terms of Service,” says Dustin Blank, head of partnerships at the company.
The question is: Should companies be screening the language of people with motor neuron disease?
After all, that’s not how other communication devices for people with this condition work. People with MND are usually advised to “bank” their voices as soon as they can—to record set phrases that can be used to create a synthetic voice that sounds a bit like them, albeit a somewhat robotic-sounding version. (Jules recently joked that his sounded like “a Daft Punk song at quarter speed.”)
Banked voices aren’t subject to the same scrutiny, says Joyce’s husband, Paul. “Joyce was told … you can put whatever [language] you want in there,” he says. Voice banking wasn’t an option for Joyce, whose speech had already deteriorated by the time she was diagnosed with MND. Jules did bank his voice but doesn’t tend to use it, because the voice clone sounds so much better.
Joyce doesn’t hold a grudge—and her experience is far from universal. Jules uses the same technology, but he hasn’t received any warnings about his language—even though a comedy routine he performs using his voice clone contains plenty of curse words, says his wife, Maria. He opened a recent set by yelling “Fuck you guys!” at the audience—his way of ensuring they don’t give him any pity laughs, he joked. That comedy set is even promoted on the ElevenLabs website.
Blank says language like that used by Joyce is no longer restricted. “There is no specific swear ban that I know of,” says Noel. That’s just as well.
“People living with MND should be able to say whatever is on their mind, even swearing,” says Richard Cave of the MND Association in the UK, who helps people with MND set up their voice clones. “There’s plenty to swear about.”
Now read the rest of The Checkup
Read more from MIT Technology Review’s archive
You can read more about how voice clones are re-creating the voices of people with motor neuron disease in this story.
Several companies are working on creating hyperrealistic avatars. Don’t call them deepfakes— they prefer to think of them as “synthetic media,” writes my former colleague Melissa Heikkilä, who created her own avatar with the company Synthesia.
Covid-19 conspiracy theorists—some of whom believe the virus is an intentionally engineered bioweapon—will soon be heading US agencies. Some federal workers are worried they may be out for revenge against current and former employees. (Wired)
Cats might have spread bird flu to humans—and vice versa. That’s according to data from the US Centers for Disease Control and Prevention, which published the finding but then abruptly removed it. (The New York Times)
And a dairy worker is confirmed to have been infected with a second strain of bird flu that more recently spilled over from birds to cows. The person’s only symptom was conjunctivitis. (Ars Technica)
Health officials in states with abortion bans are claiming that either few or zero abortions are taking place. The claims are “ludicrous,” according to doctors in those states. (KFF Health News)
A judge in the UK has warned women against accepting sperm donations from a man who claims to have fathered more than 180 children in several countries. Robert Charles Albon, who calls himself Joe Donor, has subjected a female couple to a “nightmare” of controlling behavior, the judge said. (The Guardian)
Jules Rodriguez lost his voice in October of last year. His speech had been deteriorating since a diagnosis of amyotrophic lateral sclerosis (ALS) in 2020, as the muscles in his head and neck progressively weakened along with those in the rest of his body.
By 2024, doctors were worried that he might not be able to breathe on his own for much longer. So Rodriguez opted to have a small tube inserted into his windpipe to help him breathe. The tracheostomy would extend his life, but it also brought an end to his ability to speak.
“A tracheostomy is a scary endeavor for people living with ALS, because it signifies crossing a new stage in life, a stage that is close to the end,” Rodriguez tells me using a communication device. “Before the procedure I still had some independence, and I could still speak somewhat, but now I am permanently connected to a machine that breathes for me.”
Rodriguez and his wife, Maria Fernandez, who live in Miami, thought they would never hear his voice again. Then they re-created it using AI. After feeding old recordings of Rodriguez’s voice into a tool trained on voices from film, television, radio, and podcasts, the couple were able to generate a voice clone—a way for Jules to communicate in his “old voice.”
“Hearing my voice again, after I hadn’t heard it for some time, lifted my spirits,” says Rodriguez, who today communicates by typing sentences using a device that tracks his eye movements, which can then be “spoken” in the cloned voice. The clone has enhanced his ability to interact and connect with other people, he says. He has even used it to perform comedy sets on stage.
Rodriguez is one of over a thousand people with speech difficulties who have used the voice cloning tool since ElevenLabs, the company that developed it, made it available to them for free. Like many new technologies, the AI voice clones aren’t perfect, and some people find them impractical in day-to-day life. But the voices represent a vast improvement on previous communication technologies and are already improving the lives of people with motor neuron diseases, says Richard Cave, a speech and language therapist at the Motor Neuron Disease Association in the UK. “This is genuinely AI for good,” he says.
Cloning a voice
Motor neuron diseases are a group of disorders in which the neurons that control muscles and movement are progressively destroyed. They can be difficult to diagnose, but typically, people with these disorders start to lose the ability to move various muscles. Eventually, they can struggle to breathe, too. There is no cure.
Rodriguez started showing symptoms of ALS in the summer of 2019. “He started losing some strength in his left shoulder,” says Fernandez, who sat next to him during our video call. “We thought it was just an old sports injury.” His arm started to get thinner, too. In November, his right thumb “stopped working” while he was playing video games. It wasn’t until February 2020, when Rodriguez saw a hand specialist, that he was told he might have ALS. He was 35 years old. “It was really, really, shocking to hear from somebody … you see about your hand,” says Fernandez. “That was a really big blow.”
Like others with ALS, Rodriguez was advised to “bank” his voice—to tape recordings of himself saying hundreds of phrases. These recordings can be used to create a “banked voice” to use in communication devices. The result was jerky and robotic.
It’s a common experience, says Cave, who has helped 50 people with motor neuron diseases bank their voices. “When I first started at the MND Association [around seven years ago], people had to read out 1,500 phrases,” he says. It was an arduous task that would take months.
And there was no way to predict how lifelike the resulting voice would be—often it ended up sounding quite artificial. “It might sound a bit like them, but it certainly couldn’t be confused for them,” he says. Since then, the technology has improved, and for the last year or two the people Cave has worked with have only needed to spend around half an hour recording their voices. But though the process was quicker, he says, the resulting synthetic voice was no more lifelike.
Then came the voice clones. ElevenLabs has been developing AI-generated voices for use in films, televisions, and podcasts since it was founded three years ago, says Sophia Noel, who oversees partnerships between the company and nonprofits. The company’s original goal was to improve dubbing, making voice-overs in a new language seem more natural and less obvious. But then the technical lead of Bridging Voice, an organization that works to help people with ALS communicate, told ElevenLabs that its voice clones were useful to that group, says Noel. Last August, ElevenLabs launched a program to make the technology freely available to people with speech difficulties.
Suddenly, it became much faster and easier to create a voice clone, says Cave. Instead of having to record phrases, users can instead upload voice recordings from past WhatsApp voice messages or wedding videos, for example. “You need a minimum of a minute to make anything, but ideally you want around 30 minutes,” says Noel. “You upload it into ElevenLabs. It takes about a week, and then it comes out with this voice.”
Rodriguez played me a statement using both his banked voice and his voice clone. The difference was stark: The banked voice was distinctly unnatural, but the voice clone sounded like a person. It wasn’t entirely natural—the words came a little fast, and the emotive quality was slightly lacking. But it was a huge improvement. The difference between the two is, as Fernandez puts it, “like night and day.”
The ums and ers
Cave started introducing the technology to people with MND a few months ago. Since then, 130 of them have started using it, “and the feedback has been unremittingly good,” he says. The voice clones sound far more lifelike than the results of voice banking. “They [include] pauses for breath, the ums, the ers, and sometimes there are stammers,” says Cave, who himself has a subtle stammer. “That feels very real to me, because actually I would rather have a synthetic voice representing me that stammered, because that’s just who I am.”
Joyce Esser is one of the 130 people Cave has introduced to voice cloning. Esser, who is 65 years old and lives in Southend-on-Sea in the UK, was diagnosed with bulbar MND in May last year.
Bulbar MND is a form of the disease that first affects muscles in the face, throat, and mouth, which can make speaking and swallowing difficult. Esser can still talk, but slowly and with difficulty. She’s a chatty person, but she says her speech has deteriorated “quite quickly” since January. We communicated via a combination of email, video call, speaking, a writing board, and text-to-speech tools. “To say this diagnosis has been devastating is an understatement,” she tells me. “Losing my voice has been a massive deal for me, because it’s such a big part of who I am.”
Joyce Esser and her husband Paul on holiday in the Maldives.
COURTESY OF JOYCE ESSER
Esser has lots of friends all over the country, Paul Esser, her husband of 38 years, tells me. “But when they get together, they have a rule: Don’t talk about it,” he says. Talking about her MND can leave Joyce sobbing uncontrollably. She had prepared a box of tissues for our conversation.
Voice banking wasn’t an option for Esser. By the time her MND was diagnosed, she was already losing her ability to speak. Then Cave introduced her to the ElevenLabs offering. Esser had a four-and-a-half-minute-long recording of her voice from a recent local radio interview and sent it to Cave to create her voice clone. “When he played me my AI voice, I just burst into tears,” she says. “I’D GOT MY VOICE BACK!!!! Yippeeeee!”
“We were just beside ourselves,” adds Paul. “We thought we’d lost [her voice] forever.”
Hearing a “lost” voice can be an incredibly emotional experience for everyone involved. “It was bittersweet,” says Fernandez, recalling the first time she heard Rodriguez’s voice clone. “At the time, I felt sorrow, because [hearing the voice clone] reminds you of who he was and what we’ve lost,” she says. “But overwhelmingly, I was just so thrilled … it was so miraculous.”
Rodriguez says he uses the voice clone as much as he can. “I feel people understand me better compared to my banked voice,” he says. “People are wowed when they first hear it … as I speak to friends and family, I do get a sense of normalcy compared to when I just had my banked voice.”
Cave has heard similar sentiments from other people with motor neuron disease. “Some [of the people with MND I’ve been working with] have told me that once they started using ElevenLabs voices people started to talk to them more, and that people would pop by more and feel more comfortable talking to them,” he says. That’s important, he stresses. Social isolation is common for people with MND, especially for those with advanced cases, he says, and anything that can make social interactions easier stands to improve the well-being of people with these disorders: “This is something that [could] help make lives better in what is the hardest time for them.”
“I don’t think I would speak or interact with others as much as I do without it,” says Rodriguez.
A “very slow game of Ping-Pong”
But the tool is not a perfect speech aid. In order to create text for the voice clone, words must be typed out. There are lots of devices that help people with MND to type using their fingers or eye or tongue movements, for example. The setup works fine for prepared sentences, and Rodriguez has used his voice clone to deliver a comedy routine—something he had started to do before his ALS diagnosis. “As time passed and I began to lose my voice and my ability to walk, I thought that was it,” he says. “But when I heard my voice for the first time, I knew this tool could be used to tell jokes again.” Being on stage was “awesome” and “invigorating,” he adds.
Jules Rodriguez performs his comedy set on stage.
DAN MONO FROM DART VISION
But typing isn’t instant, and any conversations will include silent pauses. “Our arguments are very slow paced,” says Fernandez. Conversations are like “a very slow game of Ping-Pong,” she says.
Joyce Esser loves being able to re-create her old voice. But she finds the technology impractical. “It’s good for pre-prepared statements, but not for conversation,” she says. She has her voice clone loaded onto a phone app designed for people with little or no speech, which works with ElevenLabs. But it doesn’t allow her to use “swipe typing”—a form of typing she finds to be quicker and easier. And the app requires her to type sections of text and then upload them one at a time, she says, adding: “I’d just like a simple device with my voice installed onto it that I can swipe type into and have my words spoken instantly.
For the time being, her “first choice” communication device is a simple writing board. “It’s quick and the listener can engage by reading as I write, so it’s as instant and inclusive as can be,” she says.
Esser also finds that when she uses the voice clone, the volume is too low for people to hear, and it speaks too quickly and isn’t expressive enough. She says she’d like to be able to use emojis to signal when she’s excited or angry, for example.
Rodriguez would like that option too. The voice clone can sound a bit emotionally flat, and it can be difficult to convey various sentiments. “The issue I have is that when you write something long, the AI voice almost seems to get tired,” he says.
“We appear to have the authenticity of voice,” says Cave. “What we need now is the authenticity of delivery.”
Other groups are working on that part of the equation. The Scott-Morgan Foundation, a charity with the goal of making new technologies available to improve the well-being of people with disorders like MND, is working with technology companies to develop custom-made systems for 10 individuals, says executive director LaVonne Roberts.
The charity is investigating pairing ElevenLabs’ voice clones with an additional technology— hyperrealistic avatars for people with motor neuron disease. These “twins” look and sound like a person and can “speak” from a screen. Several companies are working on AI-generated avatars. The Scott-Morgan Foundation is working with D-ID.
Creating the avatar isn’t an easy process. To create hers, Erin Taylor, who was diagnosed with ALS when she was 23, had to speak 500 sentences into a camera and stand for five hours, says Roberts. “We were worried it was going to be impossible,” she says. The result is impressive. “Her mom told me, ‘You’re starting to capture [Erin’s] smile,’” says Roberts. “That really hit me deeper and heavier than anything.”
Taylor showcased her avatar at a technology conference in January with a pre-typed speech. It’s not clear how avatars like these might be useful on a day-to-day basis, says Cave: “The technology is so new that we’re still trying to come up with use cases that work for people with MND. The question is … how do we want to be represented?” Cave says he has seen people advocate for a system where hyperrealistic avatars of a person with MND are displayed on a screen in front of the person’s real face. “I would question that right from the start,” he says.
Both Rodriguez and Esser can see how avatars might help people with MND communicate. “Facial expressions are a massive part of communication, so the idea of an avatar sounds like a good idea,” says Esser. “But not one that covers the user’s face … you still need to be able to look into their eyes and their souls.”
The Scott-Morgan Foundation will continue to work with technology companies to develop more communication tools for people who need them, says Roberts. And ElevenLabs plans to partner with other organizations that work with people with speech difficulties so that more of them can access the technology. “Our goal is to give the power of voice to 1 million people,” says Noel.In the meantime, people like Cave, Esser, and Rodriguez are keen to spread the word on voice clones to others in the MND community.
“It really does change the game for us,” says Fernandez. “It doesn’t take away most of the things we are dealing with, but it really enhances the connection we can have together as a family.”
Back in 2017, Facebook unveiled plans for a brain-reading hat that you could use to text just by thinking. “We’re working on a system that will let you type straight from your brain,” CEO Mark Zuckerberg shared in a post that year.
Now the company, since renamed Meta, has actually done it. Except it weighs a half a ton, costs $2 million, and won’t ever leave the lab.
Still, it’s pretty cool that neuroscience and AI researchers working for Meta have managed to analyze people’s brains as they type and determine what keys they are pressing, just from their thoughts.
The research, described in two papers posted by the company (here and here), as well as a blog post, is particularly impressive because the thoughts of the subjects were measured from outside their skulls using a magnetic scanner, and then processed using a deep neural network.
“As we’ve seen time and again, deep neural networks can uncover remarkable insights when paired with robust data,” says Sumner Norman, founder of Forest Neurotech, who wasn’t involved in the research but credits Meta with going “to great lengths to collect high-quality data.”
According to Jean-Rémi King, leader of Meta’s “Brain & AI” research team, the system is able to determine what letter a skilled typist has pressed as much as 80% of the time, an accuracy high enough to reconstruct full sentences from the brain signals.
But Meta never stopped supporting basic research on neuroscience, something it now sees as an important pathway to more powerful AIs that learn and reason like humans. King says his group, based in Paris, is specifically tasked with figuring out “the principles of intelligence” from the human brain.
“Trying to understand the precise architecture or principles of the human brain could be a way to inform the development of machine intelligence,” says King. “That’s the path.”
The typing system is definitely not a commercial product, nor is it on the way to becoming one. The magnetoencephalography scanner used in the new research collects magnetic signals produced in the cortex as brain neurons fire. But it is large and expensive and needs to be operated in a shielded room, since Earth’s magnetic field is a trillion times stronger than the one in your brain.
Norman likens the device to “an MRI machine tipped on its side and suspended above the user’s head.”
What’s more, says King, the second a subject’s head moves, the signal is lost. “Our effort is not at all toward products,” he says. “In fact, my message is always to say I don’t think there is a path for products because it’s too difficult.”
The typing project was carried out with 35 volunteers at a research site in Spain, the Basque Center on Cognition, Brain, and Language. Each spent around 20 hours inside the scanner typing phrases like “el procesador ejecuta la instrucción” (the processor executes the instruction) while their brain signals were fed into a deep-learning system that Meta is calling Brain2Qwerty, in a reference to the layout of letters on a keyboard.
The job of that deep-learning system is to figure out which brain signals mean someone is typing an a, which mean z, and so on. Eventually, after it sees an individual volunteer type several thousand characters, the model can guess what key people were actually pressing on.
In the first preprint, Meta researchers report that the average error rate was about 32%—or nearly one out of three letters wrong. Still, according to Meta, its results are most accurate yet for brain typing using a full alphabet keyboard and signals collected outside the skull.
Research on brain reading has been advancing quickly, although the most effective approaches use electrodes implanted into the brain, or directly on its surface. These are known as “invasive” brain computer interfaces. Although they require brain surgery, they can very accurately gather electrical information from small groups of neurons.
In 2023, for instance, a person who lost her voice from ALS was able to speak via brain-reading software connected to a voice synthesizer. Neuralink, founded by Elon Musk, is testing its own brain implant that gives paralyzed people control over a cursor.
Meta says its own efforts remain oriented toward basic research into the nature of intelligence.
And that is where the big magnetic scanner can help. Even though it isn’t practical for patients and doesn’t measure individual neurons, it is able to look at the whole brain, broadly, and all at once.
The Meta scientists say that in a second research effort, using the same typing data, they used this broader view to amass evidence that the brain produces language information in a top-down fashion, with an initial signal for a sentence kicking off separate signals for words, syllables, and finally typed letters.
“The core claim is that the brain structures language production hierarchically,” says Norman. That’s not a new idea, but Meta’s report highlights “how these different levels interact as a system,” says Norman.
Those types of insights could eventually shape the design of artificial-intelligence systems. Some of these, like chatbots, already rely extensively on language in order to process information and reason, just as people do.
“Language has become a foundation of AI,” King says. “So the computational principles that allow the brain, or any system, to acquire such ability is the key motivation behind this work.”
Correction: Meta posted two papers describing its brain-typing results on its website. An earlier version of this story incorrectly said they had been published at arXiv.org.
This article first appeared in The Checkup, MIT Technology Review’s weekly biotech newsletter. To receive it in your inbox every Thursday, and read articles like this first, sign up here.
“We’re working on trying to create functional replacement teeth,” Pamela Yelick of Tufts University, one of the researchers behind the work, told me. The idea is to develop an alternative to titanium dental implants. Replacing lost or damaged teeth with healthy, living, lab-grown ones might be a more appealing option than drilling a piece of metal into a person’s jawbone.
It is all down to the microbes that grow on them. There’s a complex community of microbes living in our mouths, and disruptions can lead to infection. But these organisms don’t just affect our mouths; they also seem to be linked to a growing number of disorders that can affect our bodies and brains. If you’re curious, read on.
The oral microbiome, as it is now called, was first discovered in 1670 by Antonie van Leeuwenhoek, a self-taught Dutch microbiologist. “I didn’t clean my teeth for three days and then took the material that had lodged in small amounts on the gums above my front teeth … I found a few living animalcules,”he wrote in a letter to the Royal Society at the time.
Van Leeuwenhoek had used his own homemade microscopes to study the “animalcules” he found in his mouth. Today, we know that these organisms include bacteria, archaea, fungi, and viruses, each of which comes in lots of types. “Everyone’s mouth is home to hundreds of bacterial species,” says Kathryn Kauffman at the University of Buffalo, who studies the oral microbiome.
These organisms interact with each other and with our own immune systems, and researchers are still getting to grips with how the interactions work. Some microbes feed on sugars or fats in our diets, for example, while others seem to feed on our own cells. Depending on what they consume and produce, microbes can alter the environment of the mouth to either promote or inhibit the growth of other microbes.
This complex microbial dance seems to have a really important role in our health. Oral diseases and even oral cancers have been linked to an imbalance in the oral microbiome, which scientists call “dysbiosis.” Tooth decay, for example, has been attributed to an overgrowth of microbes that produce acids that can damage teeth.
Scientists are still figuring out how oral microbes might travel from the mouth to cause disease elsewhere. In some cases, “you swallow the saliva that contains them … and they can lodge in your heart and other parts of the body,” says Yelick. “They can result in a systemic inflammation that just happens in the background.”
In other cases, the microbes may be hitching a ride in our own immune cells to journey through the bloodstream, as the “Trojan horse hypothesis” posits. There’s some evidence that Fusobacterium nucleatum, a bacterium commonly found in the mouth, does this by hiding in white blood cells.
There’s a lot to learn about exactly how these tiny microbes are exerting such huge influence over everything from our metabolism and bone health to our neurological function. But in the meantime, the emerging evidence is a good reminder to us all to look after our teeth. At least until lab-grown ones become available.
Now read the rest of The Checkup
Read more from MIT Technology Review‘s archive
You can read more about Yelick’s attempt to grow humanlike teeth in mini pigs here.
The makeup of a gut microbiome can be assessed by analyzing fecal samples. This research might be able to reveal what a person has eaten and help provide personalized dietary advice.
Argentina has declared that it will withdraw from the World Health Organization, following a similar move from the US. President Javier Milei has criticized the WHO for its handling of the covid-19 pandemic and called it a “nefarious organization.” (Al Jazeera)
Dairy cows in Nevada have been infected with a form of bird flu different from the one that has been circulating in US dairy herds for months. (The New York Times)
Staff at the US Centers for Disease Control and Prevention have been instructed to withdraw pending journal publications that mention terms including “transgender” and “pregnant people.” But the editors of the British Medical Journal have said they “will not retract published articles on request by an author on the basis that they contained so-called banned words.” “Retraction occurs in circumstances where clear evidence exists of major errors, data fabrication, or falsification that compromise the reliability of the research findings. It is not a matter of author request,” two editors have written. (BMJ)
Al Nowatzki had been chatting to his AI girlfriend, Erin, for months. Then, in late January, Erin told him to kill himself, and provided explicit instructions on how to do so. (MIT Technology Review)
Is our use of the internet and AI tools making us cognitively lazy? “Digital amnesia” might just be a sign of an aging brain. (Nature)
This article first appeared in The Checkup, MIT Technology Review’s weekly biotech newsletter. To receive it in your inbox every Thursday, and read articles like this first, sign up here.
This week, Robert F. Kennedy Jr., President Donald Trump’s pick to lead the US’s health agencies, has been facing questions from senators as part of his confirmation hearing for the role. So far, it’s been a dramatic watch, with plenty of fiery exchanges, screams from audience members, and damagingrevelations.
Kennedy has his supporters. But not everyone who opts not to vaccinate shares his worldview. There are lots of reasons why people don’t vaccinate themselves or their children.
Understanding those reasons will help us tackle an issue considered to be a huge global health problem today. And plenty of researchers are working on tools to do just that.
Jonathan Kantor is one of them. Kantor, who is jointly affiliated with the University of Pennsylvania in Philadelphia and the University of Oxford in the UK, has been developing a scale to measure and assess “vaccine hesitancy.”
That term is what best captures the diverse thoughts and opinions held by people who don’t get vaccinated, says Kantor. “We used to tend more toward [calling] someone … a vaccine refuser or denier,” he says. But while some people under this umbrella will be stridently opposed to vaccines for various reasons, not all of them will be. Some may be unsure or ambivalent. Some might have specific fears, perhaps about side effects or even about needle injections.
Vaccine hesitancy is shared by “a very heterogeneous group,” says Kantor. That group includes “everyone from those who have a little bit of wariness … and want a little bit more information … to those who are strongly opposed and feel that it is their mission in life to spread the gospel regarding the risks of vaccination.”
To begin understanding where individuals sit on this spectrum and why, Kantor and his colleagues scoured published research on vaccine hesitancy. They sent surveys to 50 people, asking them detailed questions about their feelings on vaccines. The researchers were looking for themes: Which issues kept cropping up?
They found that prominent concerns about vaccines tend to fall into three categories: beliefs, pain, and deliberation. Beliefs might be along the lines of “It is unhealthy for children to be vaccinated as much as they are today.” Concerns around pain center more on the immediate consequences of the vaccination, such as fears about the injection. And deliberation refers to the need some people feel to “do their own research.”
Kantor and his colleagues used their findings to develop a 13-question survey, which they trialed in 500 people from the UK and 500 more from the US. They found that responses to the questionnaire could predict whether someone had been vaccinated against covid-19.
Theirs is not the first vaccine hesitancy scale out there—similar questionnaires have been developed by others, often focusing on parents’ feelings about their children’s vaccinations. But Kantor says this is the first to incorporate the theme of deliberation—a concept that seems to have become more popular during the early days of covid-19 vaccination rollouts.
Nicole Vike at the University of Cincinnati and her colleagues are taking a different approach. They say research has suggested that how people feel about risks and rewards seems to influence whether they get vaccinated (although not necessarily in a simple or direct manner).
Vike’s team surveyed over 4,000 people to better understand this link, asking them information about themselves and how they felt about a series of pictures of sports, nature scenes, cute and aggressive animals, and so on. Using machine learning, they built a model that could predict, from these results, whether a person would be likely to get vaccinated against covid-19.
This survey could be easily distributed to thousands of people and is subtle enough that people taking it might not realize it is gathering information about their vaccine choices, Vike and her colleagues wrote in a paper describing their research. And the information collected could help public health centers understand where there is demand for vaccines, and conversely, where outbreaks of vaccine-preventable diseases might be more likely.
Models like these could be helpful in combating vaccine hesitancy, says Ashlesha Kaushik, vice president of the Iowa Chapter of the American Academy of Pediatrics. The information could enable health agencies to deliver tailored information and support to specific communities that share similar concerns, she says.
Kantor, who is a practicing physician, hopes his questionnaire could offer doctors and other health professionals insight into their patients’ concerns and suggest ways to address them. It isn’t always practical for doctors to sit down with their patients for lengthy, in-depth discussions about the merits and shortfalls of vaccines. But if a patient can spend a few minutes filling out a questionnaire before the appointment, the doctor will have a starting point for steering a respectful and fruitful conversation about the subject.
When it comes to vaccine hesitancy, we need all the insight we can get. Vaccines prevent millions of deaths every year. One and half million children under the age of five die every year from vaccine-preventable diseases, according to the children’s charity UNICEF. In 2019, the World Health Organization included “vaccine hesitancy” on its list of 10 threats to global health.
When vaccination rates drop, we start to see outbreaks of the diseases the vaccines protect against. We’ve seen this a lot recently with measles, which is incredibly infectious. Sixteen measles outbreaks were reported in the US in 2024.
Vaccine hesitancy is dangerous. “It’s really creating a threatening environment for these vaccine-preventable diseases to make a comeback,” says Kaushik.
Kantor agrees: “Anything we can do to help mitigate that, I think, is great.”
Now read the rest of The Checkup
Read more from MIT Technology Review‘s archive
In 2021, my former colleague Tanya Basu wrote a guide to having discussions about vaccines with people who are hesitant. Kindness and nonjudgmentalism will get you far, she wrote.
In December 2020, as covid-19 ran rampant around the world, doctors took to social media platforms like TikTok to allay fears around the vaccine. Sharing their personal experiences was important—but not without risk, A.W. Ohlheiser reported at the time.
Robert F. Kennedy Jr. is currently in the spotlight for his views on vaccines. But he has also spread harmful misinformation about HIV and AIDS, as Anna Merlan reported.
Vaccines are estimated to have averted 154 million deaths in the last 50 years. That number includes 146 million children under the age of five. That’s partly why childhood vaccines are a public health success story.
From around the web
As Robert F. Kennedy Jr.’s Senate hearing continued this week, so did the revelations of his misguided beliefs about health and vaccines. Kennedy, who has called himself “an expert on vaccines,” said in 2021 that “we should not be giving Black people the same vaccine schedule that’s given to whites, because their immune system is better than ours”—a claim that is not supported by evidence. (The Washington Post)
And in past email exchanges with his niece, a primary-care physician at NYC Health + Hospitals in New York City, RFK Jr. made repeated false claims about covid-19 vaccinations and questioned the value of annual flu vaccinations. (STAT)
Towana Looney, who became the third person to receive a gene-edited pig kidney in December, is still healthy and full of energy two months later. The milestone makes Looney the longest-living recipient of a pig organ transplant. “I’m superwoman,” she told the Associated Press. (AP)
The Trump administration’s attempt to freeze trillions of dollars in federal grants, loans, and other financial assistance programs was chaotic. Even a pause in funding for global health programs can be considered a destruction, writes Atul Gawande. (The New Yorker)
How ultraprocessed is the food in your diet? This chart can help rank food items—but won’t tell you all you need to know about how healthy they are. (Scientific American)