Why do we hear about medical breakthroughs in mice, but rarely see them translate into cures for human disease? Why do so few drugs that enter clinical trials receive regulatory approval? And why is the waiting list for organ transplantation so long? These challenges stem in large part from a common root cause: a severe shortage of ethically sourced human bodies.
It may be disturbing to characterize human bodies in such commodifying terms, but the unavoidable reality is that human biological materials are an essential commodity in medicine, and persistent shortages of these materials create a major bottleneck to progress.
This imbalance between supply and demand is the underlying cause of the organ shortage crisis, with more than 100,000 patients currently waiting for a solid organ transplant in the US alone. It also forces us to rely heavily on animals in medical research, a practice that can’t replicate major aspects of human physiology and makes it necessary to inflict harm on sentient creatures. In addition, the safety and efficacy of any experimental drug must still be confirmed in clinical trials on living human bodies. These costly trials risk harm to patients, can take a decade or longer to complete, and make it through to approval less than 15% of the time.
There might be a way to get out of this moral and scientific deadlock. Recent advances in biotechnology now provide a pathway to producing living human bodies without the neural components that allow us to think, be aware, or feel pain. Many will find this possibility disturbing, but if researchers and policymakers can find a way to pull these technologies together, we may one day be able to create “spare” bodies, both human and nonhuman.
These could revolutionize medical research and drug development, greatly reducing the need for animal testing, rescuing many people from organ transplant lists, and allowing us to produce more effective drugs and treatments. All without crossing most people’s ethical lines.
Bringing technologies together
Although it may seem like science fiction, recent technological progress has pushed this concept into the realm of plausibility. Pluripotent stem cells, one of the earliest cell types to form during development, can give rise to every type of cell in the adult body. Recently, researchers have used these stem cells to create structures that seem to mimic the early development of actual human embryos. At the same time, artificial uterus technology is rapidly advancing, and other pathways may be opening to allow for the development of fetuses outside of the body.
Such technologies, together with established genetic techniques to inhibit brain development, make it possible to envision the creation of “bodyoids”—a potentially unlimited source of human bodies, developed entirely outside of a human body from stem cells, that lack sentience or the ability to feel pain.
There are still many technical roadblocks to achieving this vision, but we have reason to expect that bodyoids could radically transform biomedical research by addressing critical limitations in the current models of research, drug development, and medicine. Among many other benefits, they would offer an almost unlimited source of organs, tissues, and cells for use in transplantation.
It could even be possible to generate organs directly from a patient’s own cells, essentially cloning someone’s biological material to ensure that transplanted tissues are a perfect immunological match and thus eliminating the need for lifelong immunosuppression. Bodyoids developed from a patient’s cells could also allow for personalized screening of drugs, allowing physicians to directly assess the effect of different interventions in a biological model that accurately reflects a patient’s own personal genetics and physiology. We can even envision using animal bodyoids in agriculture, as a substitute for the use of sentient animal species.
Of course, exciting possibilities are not certainties. We do not know whether the embryo models recently created from stem cells could give rise to living people or, thus far, even to living mice. We do not know when, or whether, an effective technique will be found for successfully gestating human bodies entirely outside a person. We cannot be sure whether such bodyoids can survive without ever having developed brains or the parts of brains associated with consciousness, or whether they would still serve as accurate models for living people without those brain functions.
Even if it all works, it may not be practical or economical to “grow” bodyoids, possibly for many years, until they can be mature enough to be useful for our ends. Each of these questions will require substantial research and time. But we believe this idea is now plausible enough to justify discussing both the technical feasibility and the ethical implications.
Ethical considerations and societal implications
Bodyoids could address many ethical problems in modern medicine, offering ways to avoid unnecessary pain and suffering. For example, they could offer an ethical alternative to the way we currently use nonhuman animals for research and food, providing meat or other products with no animal suffering or awareness.
But when we come to human bodyoids, the issues become harder. Many will find the concept grotesque or appalling. And for good reason. We have an innate respect for human life in all its forms. We do not allow broad research on people who no longer have consciousness or, in some cases, never had it.
At the same time, we know much can be gained from studying the human body. We learn much from the bodies of the dead, which these days are used for teaching and research only with consent. In laboratories, we study cells and tissues that were taken, with consent, from the bodies of the dead and the living.
Recently we have even begun using for experiments the “animated cadavers” of people who have been declared legally dead, who have lost all brain function but whose other organs continue to function with mechanical assistance. Genetically modified pig kidneys have been connected to, or transplanted into, these legally dead but physiologically active cadavers to help researchers determine whether they would work in living people.
In all these cases, nothing was, legally, a living human being at the time it was used for research. Human bodyoids would also fall into that category. But there are still a number of issues worth considering. The first is consent: The cells used to make bodyoids would have to come from someone, and we’d have to make sure that this someone consented to this particular, likely controversial, use. But perhaps the deepest issue is that bodyoids might diminish the human status of real people who lack consciousness or sentience.
Thus far, we have held to a standard that requires us to treat all humans born alive as people, entitled to life and respect. Would bodyoids—created without pregnancy, parental hopes, or indeed parents—blur that line? Or would we consider a bodyoid a human being, entitled to the same respect? If so, why—just because it looks like us? A sufficiently detailed mannequin can meet that test. Because it looks like us and is alive? Because it is alive and has our DNA? These are questions that will require careful thought.
A call to action
Until recently, the idea of making something like a bodyoid would have been relegated to the realms of science fiction and philosophical speculation. But now it is at least plausible—and possibly revolutionary. It is time for it to be explored.
The potential benefits—for both human patients and sentient animal species—are great. Governments, companies, and private foundations should start thinking about bodyoids as a possible path for investment. There is no need to start with humans—we can begin exploring the feasibility of this approach with rodents or other research animals.
As we proceed, the ethical and social issues are at least as important as the scientific ones. Just because something can be done does not mean it should be done. Even if it looks possible, determining whether we should make bodyoids, nonhuman or human, will require considerable thought, discussion, and debate. Some of that will be by scientists, ethicists, and others with special interest or knowledge. But ultimately, the decisions will be made by societies and governments.
The time to start those discussions is now, when a scientific pathway seems clear enough for us to avoid pure speculation but before the world is presented with a troubling surprise. The announcement of the birth of Dolly the cloned sheep back in the 1990s launched a hysterical reaction, complete with speculation about armies of cloned warrior slaves. Good decisions require more preparation.
The path toward realizing the potential of bodyoids will not be without challenges; indeed, it may never be possible to get there, or even if it is possible, the path may never be taken. Caution is warranted, but so is bold vision; the opportunity is too important to ignore.
Carsten T. Charlesworth is a postdoctoral fellow at the Institute of Stem Cell Biology and Regenerative Medicine (ISCBRM) at Stanford University.
Henry T. Greely is the Deane F. and Kate Edelman Johnson Professor of Law and director of the Center for Law and the Biosciences at Stanford University.
Hiromitsu Nakauchi is a professor of genetics and an ISCBRM faculty member at Stanford University and a distinguished university professor at the Institute of Science Tokyo.
Over the past couple of weeks, I’ve been following news of the deaths of actor Gene Hackman and his wife, pianist Betsy Arakawa. It was heartbreaking to hear how Arakawa appeared to have died from a rare infection days before her husband, who had advanced Alzheimer’s disease and may have struggled to understand what had happened.
But as I watched the medical examiner reveal details of the couple’s health, I couldn’t help feeling a little uncomfortable. Media reports claim that the couple liked their privacy and had been out of the spotlight for decades. But here I was, on the other side of the Atlantic Ocean, being told what pills Arakawa had in her medicine cabinet, and that Hackman had undergone multiple surgeries.
It made me wonder: Should autopsy reports be kept private? A person’s cause of death is public information. But what about other intimate health details that might be revealed in a postmortem examination?
The processes and regulations surrounding autopsies vary by country, so we’ll focus on the US, where Hackman and Arakawa died. Here, a “medico-legal” autopsy may be organized by law enforcement agencies and handled through courts, while a “clinical” autopsy may be carried out at the request of family members.
And there are different levels of autopsy—some might involve examining specific organs or tissues, while more thorough examinations would involve looking at every organ and studying tissues in the lab.
The goal of an autopsy is to discover the cause of a person’s death. Autopsy reports, especially those resulting from detailed investigations, often reveal health conditions—conditions that might have been kept private while the person was alive. There are multiple federal and state laws designed to protect individuals’ health information. For example, the Health Insurance Portability and Accountability Act (HIPAA) protects “individually identifiable health information” up to 50 years after a person’s death. But some things change when a person dies.
For a start, the cause of death will end up on the death certificate. That is public information. The public nature of causes of death is taken for granted these days, says Lauren Solberg, a bioethicist at the University of Florida College of Medicine. It has become a public health statistic. She and her student Brooke Ortiz, who have been researching this topic, are more concerned about other aspects of autopsy results.
The thing is, autopsies can sometimes reveal more than what a person died from. They can also pick up what are known as incidental findings. An examiner might find that a person who died following a covid-19 infection also had another condition. Perhaps that condition was undiagnosed. Maybe it was asymptomatic. That finding wouldn’t appear on a death certificate. So who should have access to it?
The laws over who should have access to a person’s autopsy report vary by state, and even between counties within a state. Clinical autopsy results will always be made available to family members, but local laws dictate which family members have access, says Ortiz.
Genetic testing further complicates things. Sometimes the people performing autopsies will run genetic tests to help confirm the cause of death. These tests might reveal what the person died from. But they might also flag genetic factors unrelated to the cause of death that might increase the risk of other diseases.
In those cases, the person’s family members might stand to benefit from accessing that information. “My health information is my health information—until it comes to my genetic health information,” says Solberg. Genes are shared by relatives. Should they have the opportunity to learn about potential risks to their own health?
This is where things get really complicated. Ethically speaking, we should consider the wishes of the deceased. Would that person have wanted to share this information with relatives?
It’s also worth bearing in mind that a genetic risk factor is often just that; there’s often no way to know whether a person will develop a disease, or how severe the symptoms would be. And if the genetic risk is for a disease that has no treatment or cure, will telling the person’s relatives just cause them a lot of stress?
One 27-year-old experienced this when a 23&Me genetic test told her she had “a 28% chance of developing late-onset Alzheimer’s disease by age 75 and a 60% chance by age 85.”
“I’m suddenly overwhelmed by this information,” she posted on a dementia forum. “I can’t help feeling this overwhelming sense of dread and sadness that I’ll never be able to un-know this information.”
In their research, Solberg and Ortiz came across cases in which individuals who had died in motor vehicle accidents underwent autopsies that revealed other, asymptomatic conditions. One man in his 40s who died in such an accident was found to have a genetic kidney disease. A 23-year-old was found to have had kidney cancer.
Ideally, both medical teams and family members should know ahead of time what a person would have wanted—whether that’s an autopsy, genetic testing, or health privacy. Advance directives allow people to clarify their wishes for end-of-life care. But only around a third of people in the US have completed one. And they tend to focus on care before death, not after.
Solberg and Ortiz think they should be expanded. An advance directive could specify how people want to share their health information after they’ve died. “Talking about death is difficult,” says Solberg. “For physicians, for patients, for families—it can be uncomfortable.” But it is important.
On March 17, a New Mexico judge granted a request from a representative of Hackman’s estate to seal police photos and bodycam footage as well as the medical records of Hackman and Arakawa. The medical investigator is “temporarily restrained from disclosing … the Autopsy Reports and/or Death Investigation Reports for Mr. and Mrs. Hackman,” according to Deadline.
This article first appeared in The Checkup, MIT Technology Review’s weekly biotech newsletter. To receive it in your inbox every Thursday, and read articles like this first, sign up here.
Around 1,400 infants are being infected by HIV every day as a result of the new US administration’s cuts to funding to AIDS organizations, new modeling suggests.
In an executive order issued January 20, President Donald Trump paused new foreign aid funding to global health programs, and four days later, US Secretary of State Marco Rubio issued a stop-work order on existing foreign aid assistance. Surveys suggest that these changes forced more than a third of global organizations that provide essential HIV services to close within days of the announcements.
Hundreds of thousands of people are losing access to HIV treatments as a result. Women and girls are missing out on cervical cancer screening and services for gender-based violence, too. A waiver Rubio later issued in an attempt to restore lifesaving services has had very little impact.
“We are in a crisis,” said Jennifer Sherwood, director of research, public policy, at amfAR, the Foundation for AIDS Research, at a data-sharing event on March 17 at Columbia University in New York. “Even funds that had already been appropriated, that were in the field, in people’s bank accounts, [were] frozen.”
Rubio approved a waiver for “life-saving” humanitarian assistance on January 28. “This resumption is temporary in nature, and with limited exceptions as needed to continue life-saving humanitarian assistance programs, no new contracts shall be entered into,” he said in a statement at the time.
The US President’s Emergency Plan for AIDS Relief (PEPFAR), which invests millions of dollars in the global AIDS response every year, was also granted a waiver February 1 to continue “life-saving” work.
Despite this waiver, there have been devastating reports of the impact on health programs across the many low-income countries that relied on the US Agency for International Development (USAID), which oversees PEPFAR, for funding. To get a better sense of the overall impact, amfAR conducted two surveys looking at more than 150 organizations that rely on PEPFAR funding in more than 26 countries.
“We found really severe disruptions to HIV services,” said Sherwood, who presented the findings at Columbia. “About 90% of our participants said [the cuts] had severely limited their ability to deliver HIV services.” Specifically, 94% of follow-up services designed to monitor people’s progress were either canceled or disrupted. There were similarly dramatic disruptions to services for HIV testing, treatment, and prevention, and 92% of services for gender-based violence were canceled or disrupted.
The cuts have plunged organizations into a “deep financial crisis,” said Sherwood. Almost two-thirds of respondents said community-based staff were laid off before the end of January. When the team asked these organizations how long they could stay open without US funding, 36% said they had already closed. “Only 14% said that they were able to stay open longer than a month,” said Sherwood. “And … this data was collected longer than a month ago.”
The organizations said tens of thousands of the people they serve would lose HIV treatment within a month. For some organizations, that figure was over 100,000, said Sherwood.
Part of the problem is that the stop-work order came at a time when these organizations were already experiencing “shortages in commodities,” Sherwood said. Typically, centers might give a person a six-month supply of antiretroviral drugs. Before the stop-work order, many organizations were only giving one-month supplies. “Almost all of their clients are due to come back and pick up [more] treatments in this 90-day freeze,” she said. “You can really see the panic this has caused.”
The waiver for “life-saving” treatment didn’t do much to remedy this situation. Only 5% of the organizations received funds under the waiver, while the vast majority either were told they didn’t qualify or had not been told they could restart services. “While the waiver might be one important avenue to restart some services, it cannot, on the whole, save the US HIV program,” says Sherwood. “It is very limited in scope, and it has not been widely communicated to the field.”
AmfAR isn’t the only organization tracking the impact of US funding cuts. At the same event, Sara Casey, assistant professor of population and family health at Columbia, presented results of a survey of 101 people who work in organizations reliant on US aid. They reported seeing disruptions to services in humanitarian responses, gender-based violence, mental health, infectious diseases, essential medicines and vaccines, and more. “Many of these should have been eligible for the ‘life-saving’ waivers,” Casey said.
Casey and her colleagues have also been interviewing people in Colombia, Kenya, and Nepal. In those countries, women of reproductive age, newborns and children, people living with HIV, members of the LGBTQI+ community, and migrants are among those most affected by the cuts, she said, and health workers, who are primarily women, are losing their livelihoods.
“There will be really disproportionate impacts on the world’s most vulnerable,” said Sherwood. Women make up 67% of the health-care workforce, according to the World Health Organization. They also make up 63% of PEPFAR clients. PEPFAR has supported gender equality and services for gender-based violence. “We don’t know if other countries or other donors … can or will pick up these types of programs, especially in the face of competing priorities about keeping people on treatment and keeping people alive,” said Sherwood.
Sherwood and her colleagues at amfAR have also done some modeling work to determine the potential impact of cuts to PEPFAR on women and girls, using data from last year to create their estimates. “Each day that the stop-work order is in place, we estimate that there are 1,400 new HIV infections among infants,” she said. And every day, over 7,000 women stand to miss out on cervical cancer screenings.
The funding cuts have also had a dramatic effect on mental-health services, said Farah Arabe, who serves on the advisory board of the Global Mental Health Action Network. Arabe presented the preliminary findings of an ongoing survey of mental-health organizations from 29 countries that receive US aid. “Unfortunately, this is a very grim picture,” she said. “Only 5% of individuals who were receiving services in 2024 will be able to receive services in 2025.”
The same goes for children and adolescents. “This is a particularly sad picture because children … are going through brain development,” she said. “Impacts … at this early stage of life have lifelong impacts on academic achievement, economic productivity, mental health, physical health … even the ability to parent the next generation.”
For now, nonprofits and aid and research organizations are scrambling to try to understand, and potentially limit, the impact of the cuts. Some are hoping to locate new sources of funding, independent of the US.
“I am deeply concerned that progress in disease eradication, poverty reduction, and gender equality is at risk of being reversed,” said Thoai Ngo of Columbia University’s Mailman School of Public Health, who chaired the event. “Without urgent action, preventable deaths will rise, more people will fall into poverty, and as always, women and girls will bear the heaviest burden.”
On March 10, Rubio announced the results of his department’s review of USAID. “After a 6 week review we are officially cancelling 83% of the programs at USAID,” he shared via the social media platform X.
This article first appeared in The Checkup, MIT Technology Review’s weekly biotech newsletter. To receive it in your inbox every Thursday, and read articles like this first, sign up here.
You never hear “100%” in medicine. The trial was the most successful we’ve ever seen for HIV prevention. The drug was safe, too (it’s already approved to treat HIV infections). And it only needed to be injected twice a year to offer full protection.
This week, the results of a small phase I trial for once-yearly lenacapavir injections were announced at a conference in San Francisco. These early “first in human” trials are designed to test the safety of a drug in healthy volunteers. Still, the results are incredibly promising: All the volunteers still had the drug in their blood plasma a year after their injections, and at levels that earlier studies suggest will protect them from HIV infections.
I don’t normally get too excited about phase I trials, which usually involve just a handful of volunteers and typically don’t tell us much about whether a drug is likely to work. But this trial seems to be different. Together, the lenacapavir trials could bring us a significant step closer to ending the HIV epidemic.
First, a quick recap. We’ve had effective pre-exposure prophylactic (PrEP) drugs for HIV since 2012, but these must be taken either daily or just before a person is exposed to the virus. In 2021, the US Food and Drug Administration approved the first long-acting injectable drug for HIV prevention. That drug, cabotegravir, needs to be injected every two months.
But researchers have been working on drugs that offer even longer-lasting protection. It can be difficult for people to remember to take daily pills when they’re sick, let alone when they’re healthy. And these medicines have a stigma attached to them. “People are concerned about people hearing the pills shake in their purse on the bus … or seeing them on a medicine cabinet or bedside table,” says Moupali Das, vice president of HIV prevention and virology, pediatrics, and HIV clinical development at Gilead Sciences.
Then came the lenacapavir studies. The drug is already approved as a treatment for some cases of HIV infection, but two trials last year tested its effectiveness at prevention. In one, over 5,000 women and adolescent girls in Uganda and South Africa received either twice-yearly injections of lenacapavir or a daily PrEP pill. That trial was a resounding success: There were no cases of HIV among the volunteers who got lenacapavir.
In the most recent study, which was also published in The Lancet, Das and her colleagues tested a new formulation of the drug in 40 healthy volunteers in the US. The participants still got lenacapavir, but in a slightly different formulation, and at a higher dose. And whereas the previous trials involved injections under the skin, these participants received injections into their glute muscles. Half the volunteers in this trial received a higher dose than the others.
The drug appeared to be safe. It also appears likely to be effective. These individuals weren’t at risk of HIV. But the levels of the drug in their blood plasma remained high, even in the people who got the lower dose.
A year after their injection, the levels of the drug were still higher than those seen in people who were protected from HIV in last year’s trials. This suggests the new annual shot will be just as protective as the twice-yearly shot, says Renu Singh, a senior director in clinical pharmacology at Gilead Sciences, who presented the findings at the Conference on Retroviruses and Opportunistic Infections in San Francisco.
“I was just so excited [to hear the results],” says Carina Marquez, an associate professor of medicine at the University of California, San Francisco, who both studies infectious disease and treats people with HIV.
Annual shots would make things easier—and potentially cheaper—for both patients and health-care providers, says Marquez. “It will be a game changer if it works, which looks promising from the phase I data,” she says.
The drug works by interfering with the virus’s ability to replicate. But it also seems to have some very unusual properties, says Singh. It can be taken daily or yearly. Small doses can stay in the blood for days rather than hours. And bigger doses form what’s known as a depot, which gradually releases the drug over time.
“I previously worked at the FDA, and looked at many, many different molecules and products, but I’ve never seen [anything] like this,” Singh adds. She and her colleagues have come up with nicknames for the drug, including “magical,” “the unicorn,” and “limitless len.”
Once a phase I trial is successfully completed, researchers will typically move on to a phase II trial, which is designed to test the efficacy of a drug. That’s not necessary for lenacapavir, given the unprecedented success of last year’s trials. The team at Gilead is currently planning a phase III trial, which will involve testing annual shots in large numbers of people at risk of HIV infection.
The drug isn’t approved yet, but the researchers at Gilead have submitted twice-yearly lenacapavir for approval by the FDA and the European Medicines Agency and hope to have it approved by the FDA in June, says Das. The drug is also being assessed under the EU-Medicines for all (EU-M4all) procedure, which is a collaboration between the EMA and the World Health Organizations to fast-track the approval of drugs for countries outside Europe.
With any new medicine for an infection that affects low- and middle-income countries, there are always concerns about cost. The existing formulations of lenacapvir (used for treating HIV infections) can cost around $40,000 for a year’s supply. “There’s no price for the twice-yearly [formulation] yet,” says Das.
But this was an effort coordinated with the US President’s Emergency Plan for AIDS Relief (PEPFAR), a program whose very existence has come under threat following an executive order issued by the Trump administration to pause foreign aid.
“We are looking at the political situation right now and evaluating our possible options,” says Singh. “We are committed to working with the government to see what’s next and what can be done.”
“We’re in such a good place to end the epidemic,” says Marquez. “We’ve come so far … we’ve got to go the last mile and get the product out there to the people that need it.”
Now read the rest of The Checkup
Read more from MIT Technology Review‘s archive
You can read more about why twice-yearly lenacapavir made our 2025 list of the top 10 breakthrough technologies here. (It’s also worth checking out the full list, here!)
The first approved mRNA vaccines were for covid-19. But Moderna, the pharmaceutical company behind some of those vaccines, is now working on a similar approach for HIV.
AIDS denialism is undergoing a resurgence thanks to conspiracy-theory-promoting podcasts and books, one of which was authored by the newly appointed US secretary of health and human services, Robert F. Kennedy Jr.
From around the web
Last week, I covered the creation of the “woolly mouse,” an animal with woolly-mammoth-like features. Its creators think they’re a step closer to bringing the mammoths back from extinction. But the woolly mammoth is just one of a list of animals scientists have been trying to “de-extinct.” The full list includes dodos, passenger pigeons, and even a frog that “gives birth” by vomiting babies out of its mouth. (Discover Wildlife)
The biotechnology company Beam Therapeutics claims to have corrected a DNA mutation in people with an incurable genetic disease that can affect the liver and lungs. It is the first time a mutated gene has been restored to normal, the team says. (New York Times)
In the peak covid-19 era of 2020, Jay Bhattacharya was considered a “fringe epidemiologist” by Francis Collins, then director of the US National Institutes of Health. Now, Collins is out and Bhattacharya may soon take his place. What happens when the “fringe” is in charge? (The Atlantic)
The Trump administration withdrew the nomination of Dave Weldon to run the Centers for Disease Control and Prevention. Weldon has a long track record of criticizing vaccines. (STAT)
Mississippi became the third US state to ban lab-grown meat. The state’s agriculture commissioner has written that he wants his steak to come from “farm-raised beef, not a petri dish from a lab.” (Wired)
This article first appeared in The Checkup, MIT Technology Review’s weekly biotech newsletter. To receive it in your inbox every Thursday, and read articles like this first, sign up here.
This week saw the release of some fascinating news about some very furry rodents—so-called “woolly mice”—created as part of an experiment to explore how we might one day resurrect the woolly mammoth.
The idea of bringing back extinct species has gained traction thanks to advances in sequencing of ancient DNA. In recent years, scientists have recovered genetic blueprints from the remains of dodo birds, more than 10,000 prehistoric humans, and frozen mammoths, a species that went extinct around 2000 BCE.
This ancient genetic data is deepening our understanding of the past—for instance, by shedding light on interactions among prehistoric humans. But researchers are becoming more ambitious. Rather than just reading ancient DNA, they want to use it—by inserting it into living organisms.
Colossal Biosciences, the biotech company behind the woolly mice, says that’s its plan. The eventual goal is to modify elephants with enough mammoth DNA to result in something resembling the extinct pachyderm.
To be sure, there is a long way to go. The mice Colossal created include several genetic changes previously known to make mice furry or long-haired. That is, the changes were mammoth-like, but not from a mammoth. In fact, only a single letter of uniquely mammoth DNA was added to the mice.
Because this idea is so new and attracting so much attention, I decided it would be useful to create a record of previous attempts to add extinct DNA to living organisms. And since the technology doesn’t have a name, let’s give it one: “chronogenics.”
“Examples are exceptionally few currently,” says Ben Novak, lead scientist at Revive & Restore, an organization that applies genetic technology to conservation efforts. Novak helped me track down examples, and I also got ideas from Harvard geneticist George Church—who originally envisioned the mammoth project—as well as Beth Shapiro, lead scientist at Colossal.
The starting point for chronogenics appears to be in 2004. That year, US scientists reported they’d partly re-created the deadly 1918 influenza virus and used it to infect mice. After a long search, they had retrieved examples of the virus from a frozen body in Alaska, which had preserved the germ like a time capsule. Eventually, they were able to reconstruct the entire virus—all eight of its genes—and found it had lethal effects on rodents.
This was an alarming start to the idea of gene de-extinction. As we know from movies like The Thing, digging up frozen creatures from the ice is a bad idea. Many scientists felt that recovering the 1918 flu—which had killed 30 million people—created an unnecessary risk that the virus could slip loose, setting off a new outbreak.
Viruses are not considered living things. But for the first example of chronogenics involving animals, we have to wait only until 2008, when Australian researchers Andrew Pask and Marilyn Renfree collected genetic data from a Tasmanian tiger, or thylacine, that had been kept in a jar of ethanol (the last of these carnivorous marsupials died in a Hobart zoo in 1936).
The Australians then added a short fragment of the extinct animal’s DNA to mice and showed it could regulate the activity of another gene. This was, at one level, an entirely routine study of gene function. Scientists often make DNA changes to mice to see what happens.
The difference here was that they were studying extinct genes, which they estimated accounts for 99% of the genetic diversity that has ever existed. The researchers used almost religious language to describe where the DNA had come from.
“Genetic information from an extinct species can be resurrected,” they wrote. “And in doing so, we have restored to life the genetic potential of a fragment of this extinct mammalian genome.”
That brings us to what I think is the first commercial effort to employ extinct genes, which came to our attention in 2016. Gingko Bioworks, a synthetic-biology company, started hunting in herbariums for specimens of recently extinct flowers, like one that grew on Maui’s lava fields until the early 20th century. Then the company isolated some of the genes responsible for their scent molecules.
“We did in fact insert the genes into yeast strains and measure the molecules,” says Christina Agapakis, Gingko’s former senior vice president for creative and marketing, who led the project. Ultimately, though, Ginkgo worked with a “smell artist” to imitate those odors using commercially available aroma chemicals. This means the resulting perfumes (which are for sale) use extinct genes as “inspiration,” not as actual ingredients.
That’s a little bit similar to the woolly mouse project. Some scientists complained this week that when, or if, Colossal starts to chrono-engineer elephants, it won’t really be able to make all the thousands of DNA changes needed to truly re-create the appearance and behavior of a mammoth. Instead, the result will be just “a crude approximation of an extinct creature,” one scientist said.
Agapakis suggests not being too literal-minded about gene retrieval from the past. “As an artwork, I saw how the extinct flower made different people feel a deep connection with nature, a sadness and loss at something gone forever, and a hope for a different kind of relationship to nature in the future,” she says. “So I do think there is a very powerful and poetic ethical and social component here, a demand that we care for these woolly creatures and for our entanglements with nature more broadly.”
To wrap up our short list of known efforts at chronogenics, we found only a few more examples. In 2023, a Japanese team added a single mutation found in Neanderthals to mice, to study how it changed their anatomy. And in unpublished research, a research group at Carlsberg Laboratory, in Copenhagen, says it added a genetic mutation to barley plants after sifting through 2-million-year-old DNA recovered from a mound in Greenland.
That change, to a light-receptor gene, could make the crop tolerant to the Arctic’s extremely long summer days and winter nights.
Now read the rest of The Checkup
Read more from MIT Technology Review’s archive
How many genetic edits can be made to a cell before it expires? The answer is going to be important if you want to turn an elephant into a mammoth. In 2019, scientists set a record with more than13,000 edits in one cell.
We covered a project in Denmark where ancient DNA was replicated in a barley plant. It’s part of a plan to adapt crops to grow in higher latitudes—a useful tool as the world heats up.
To learn more about prehistoric animals, some paleontologists are building robotic models that fly, swim, and slither around. For more, have a look at this MIT Technology Reviewstoryby Shi En Kim.
The researcher who discovered how to make a mouse with extra-long hair, back in 1994, is named Jean Hebert. Last year we profiled Hebert’s idea for staying young by “gradually” replacing your brain with substitute tissue.
Looking for an unintended consequence of genetic engineering? Last year, journalist Douglas Main reported how the use of GMO crops has caused the evolution of weeds resistant to herbicides.
From around the web
The United Kingdom now imports half the donor sperm used in IVF procedures. An alleged donor “shortage” is causing sperm to become more expensive than beluga caviar, on a per-gram basis. (Financial Times)
Jason Bannan, the agent who led the FBI’s scientific investigation into the origins of covid-19, is speaking out on why he thinks the pandemic was started by a lab accident in China. (Vanity Fair)
An Australian company, Cortical Labs, released what it’s calling “the first commercial biological computer.” The device combines silicon chips with thousands of human neurons. (Boing Boing)
The Trump administration is terminating medical research grants that focus on gender identity, arguing that such studies are “often unscientific” and ignore “biological realities.” Researchers vowed to press on. (Inside Medicine).
The US Senate held confirmation hearings for Stanford University doctor Jay Bhattacharya to be director of the National Institutes of Health, which funds nearly $48 billion in research each year. Bhattacharya gained prominence during the covid-19 pandemic for opposing lockdowns. (NPR)
Francis Collins has retired from the National Institutes of Health. The widely admired geneticist spent 12 years as director of the agency, through 2021, and before that he played a key role in the Human Genome Project. Early in his career he identified the gene that causes cystic fibrosis. (New York Times)
They’re small, fluffy, and kind of cute, but these mice represent a milestone in de-extinction efforts, according to their creators. The animals have undergone a series of genetic tweaks that give them features similar to those of woolly mammoths—and their creation may bring scientists a step closer to resurrecting the giant animals that roamed the tundra thousands of years ago.
“It’s a big deal,” says Beth Shapiro, chief science officer at Colossal Biosciences, the company behind the work. Scientists at Colossal have been working to “de-extinct” the woolly mammoth since the company was launched four years ago. Now she and her colleagues have shown they can create healthy animals that look the way the team wants them to look, she says.
“The Colossal woolly mouse marks a watershed moment in our de-extinction mission,” company cofounder Ben Lamm said in a statement. “This success brings us a step closer to our goal of bringing back the woolly mammoth.”
Colossal’s researchers say their ultimate goal is not to re-create a woolly mammoth wholesale. Instead, the team is aiming for what they call “functional de-extinction”—creating a mammoth-like elephant that can survive in something like the extinct animal’s habitat and potentially fulfill the role it played in that ecosystem. Shapiro and her colleagues hope that an “Arctic-adapted elephant” might make that ecosystem more resilient to climate change by helping to spread the seeds of plants, for example.
But other experts take a more skeptical view. Even if they succeed in creating woolly mammoths, or something close to them, we can’t be certain that the resulting animals will benefit the ecosystem, says Kevin Daly, a paleogeneticist at University College Dublin and Trinity College Dublin. “I think this is a very optimistic view of the potential ecological effects of mammoth reintroduction, even if everything goes to plan,” he says. “It would be hubristic to think we might have a complete grasp on what the introduction of a species such as the mammoth might do to an environment.”
Mice and mammoths
Woolly mammoth DNA has been retrieved from freeze-dried remains of animals that are tens of thousands of years old. Shapiro and her colleagues plan to eventually make changes to the genomes of modern-day elephants to make them more closely resemble those ancient mammoth genomes, in the hope that the resulting animals will look and behave like their ancient counterparts.
Before the team begins tinkering with elephants, Shapiro says, she wants to be confident that these kinds of edits work and are safe in mice. After all, Asian elephants, which are genetically related to woolly mammoths, are endangered. Elephants also have a gestation period of 22 months, which will make research slow and expensive. The gestation period of a mouse, on the other hand, is a mere 20 days, says Shapiro. “It makes [research] a lot faster.”
There are other benefits to starting in mice. Scientists have been closely studying the genetics of these rodents for decades. Shapiro and her colleagues were able to look up genes that have already been linked to wavy, long, and light-colored fur, as well as lipid metabolism. They made a shortlist of such genes that were also present in woolly mammoths but not in elephants.
The team identified 10 target genes in total. All were mouse genes but were thought to be linked to mammoth-like features. “We can’t just put a mammoth gene into a mouse,” says Shapiro. “There’s 200 million years of evolutionary divergence between them.”
Shapiro and her colleagues then carried out a set of experiments that used CRISPR and other gene-editing techniques to target these genes in groups of mice. In some cases, the team directly altered the genomes of mouse embryos before transferring them to surrogate mouse mothers. In other cases, they edited cells and injected the resulting edited cells into early-stage embryos before implanting them into other surrogates.
In total, 34 pups were born with varying numbers of gene edits, depending on which approach was taken. All of them appear to be healthy, says Shapiro. She and her colleagues will publish their work at the preprint server bioRxiv, and it has not yet been peer-reviewed.
COLOSSAL
“It’s an important proof of concept for … the reintroduction of extinct genetic variants in living [animal groups],” says Linus Girdland Flink, a specialist in ancient DNA at the University of Aberdeen, who is not involved in the project but says he supports the idea of de-extinction.
The mice are certainly woolly. But the team don’t yet know if they’d be able to survive in the cold, harsh climates that woolly mammoths lived in. Over the next year, Shapiro and her colleagues plan to investigate whether the gene edits “conferred anything other than cuteness,” she says. The team will feed the mice different diets and expose them to various temperatures in the lab to see how they respond.
Back from the brink
Representatives of Colossal have said that they plan to create a woolly mammoth by 2027 or 2028. At the moment, the team is considering 85 genes of interest. “We’re still working to compile the ultimate list,” says Shapiro. The resulting animal should have tusks, a big head, and strong neck muscles, she adds.
Given the animal’s long gestation period, reaching a 2028 deadline would mean implanting an edited embryo into an elephant surrogate in the next year or so. Shapiro says that the team is “on track” to meet this target but adds that “there’s 22 months of biology that’s really out of our control.”
That timeline is optimistic, to say the least. The target date has already been moved by a year, and the company had originally hoped to have resurrected the thylacine by 2025. Daly, who is not involved in the study, thinks the birth of a woolly mammoth is closer to a decade away.
In any case, if the project is eventually successful, the resulting animal won’t be 100% mammoth: it will be a new animal. And it is impossible to predict how it will behave and interact with its environment, says Daly.
“When you watch Jurassic Park, you see dinosaurs … as we imagine they would have been, and how they might have interacted with each other in the past,” he says. “In reality, biology is incredibly complicated.” An animal’s behavior is shaped by everything from the embryo’s environment and the microbes it encounters at birth to social interactions. “All of those things are going to be missing for a de-extinct animal,” says Daly.
It is also difficult to predict how we’ll respond to a woolly mammoth. “Maybe we’ll just treat them as [tourist attractions], and ruin any kind of ecological benefits that they might have,” says Daly. Colossal’s director of species conservation told MIT Technology Review in 2022 that the company might eventually sell tickets to see its de-extinct animals.
The team at Colossal is also working on projects to de-extinct the dodo as well as the thylacine. In addition, team members are interested in using biotech to help conservation of existing animals that are at risk of extinction. When a species dwindles, the genetic pool can shrink. This has been the fate of the pink pigeon, a genetic relative of the dodo that lives in Mauritius. The number of pink pigeons is thought to have shrunk to about 10 individuals twice in the last century.
A lack of genetic diversity can leave a species prone to disease. Shapiro and her colleagues are looking for more genetic diversity in DNA from museum specimens. They hope to be able to “edit diversity” back into the genome of the modern-day birds.
The Hawaiian honeycreeper is especially close to Shapiro’s heart. “The honeycreepers are in danger of becoming extinct because we [humans] introduced avian malaria into their habitat, and they don’t have a way to fight [it],” she says. “If we could come up with a way to help them to be resistant to avian malaria, then that will give them a chance at survival.”
Girdland Flink, of the University of Aberdeen, is more interested in pigs. Farmed pigs have also lost a lot of genetic diversity, he says. “The genetic ancestry of modern pigs looks nothing like the genetic ancestry of the earliest domesticated pigs,” he says. Pigs are vulnerable to plenty of viral strains and are considered to be “viral incubators.” Searching the genome of ancient pig remains for extinct—and potentially beneficial—genetic variants might provide us with ways to make today’s pigs more resilient to disease.
“The past is a resource that can be harnessed,” he says.
This article first appeared in The Checkup, MIT Technology Review’s weekly biotech newsletter. To receive it in your inbox every Thursday, and read articles like this first, sign up here.
This week I’ve been working on a story about a brain of glass. About five years ago, archaeologists found shiny black glass fragments inside the skull of a man who died in the Mount Vesuvius eruption of 79 CE. It seems they are pieces of brain, turned to glass.
Scientists have found ancient brains before—some are thought to be at least 10,000 years old. But this is the only time they’ve seen a brain turn to glass. They’ve even been able to spot neurons inside it.
The man’s remains were found at Herculaneum, an ancient city that was buried under meters of volcanic ash following the eruption. We don’t know if there are any other vitrified brains on the site. None have been found so far, but only about a quarter of the city has been excavated.
Some archaeologists want to continue excavating the site. But others argue that we need to protect it. Further digging will expose it to the elements, putting the artifacts and remains at risk of damage. You can only excavate a site once, so perhaps it’s worth waiting until we have the technology to do so in the least destructive way.
After all, there are some pretty recent horror stories of excavations involving angle grinders, and of ancient body parts ending up in garages. Future technologies might eventually make our current approaches look similarly barbaric.
The inescapable fact of fields like archaeology or paleontology is this: When you study ancient remains, you’ll probably end up damaging them in some way. Take, for example, DNA analysis. Scientists have made a huge amount of progress in this field. Today, geneticists can crack the genetic code of extinct animals and analyze DNA in soil samples to piece together the history of an environment.
But this kind of analysis essentially destroys the sample. To perform DNA analysis on human remains, scientists typically cut out a piece of bone and grind it up. They might use a tooth. But once it has been studied, that sample is gone for good.
Archaeological excavations have been performed for hundreds of years, and as recently as the 1950s, it was common for archaeologists to completely excavate a site they discovered. But those digs cause damage too.
Nowadays, when a site is discovered, archaeologists tend to focus on specific research questions they might want to answer, and excavate only enough to answer those questions, says Karl Harrison, a forensic archaeologist at the University of Exeter in the UK. “We will cross our fingers, excavate the minimal amount, and hope that the next generation of archaeologists will have new, better tools and finer abilities to work on stuff like this,” he says.
In general, scientists have also become more careful with human remains. Matteo Borrini, a forensic anthropologist at Liverpool John Moores University in the UK, curates his university’s collection of skeletal remains, which he says includes around 1,000 skeletons of medieval and Victorian Britons. The skeletons are extremely valuable for research, says Borrini, who himself has investigated the remains of one person who died from exposure to phosphorus in a match factory and another who was murdered.
When researchers ask to study the skeletons, Borrini will find out whether the research will somehow alter them. “If there is destructive sampling, we need to guarantee that the destruction will be minimal, and that there will be enough material [left] for further study,” he says. “Otherwise we don’t authorize the study.”
If only previous generations of archaeologists had taken a similar approach. Harrison told me the story of the discovery of “St Bees man,” a medieval man found in a lead coffin in Cumbria, UK, in 1981. The man, thought to have died in the 1300s, was found to be extraordinarily well preserved—his skin was intact, his organs were present, and he even still had his body hair.
Normally, archaeologists would dig up such ancient specimens with care, using tools made of natural substances like stone or brick, says Harrison. Not so for St Bees man. “His coffin was opened with an angle grinder,” says Harrison. The man’s body was removed and “stuck in a truck,” where he underwent a standard modern forensic postmortem, he adds.
“His thorax would have been opened up, his organs [removed and] weighed, [and] the top of his head would have been cut off,” says Harrison. Samples of the man’s organs “were kept in [the pathologist’s] garage for 40 years.”
If St Bees man were discovered today, the story would be completely different. The coffin itself would be recognized as a precious ancient artifact that should be handled with care, and the man’s remains would be scanned and imaged in the least destructive way possible, says Harrison.
Even Lindow man, who was discovered a mere three years later in nearby Manchester, got better treatment. His remains were found in a peat bog, and he is thought to have died over 2,000 years ago. Unlike poor St Bees man, he underwent careful scientific investigation, and his remains took pride of place in the British Museum. Harrison remembers going to see the exhibit when he was 10 years old.
Harrison says he’s dreaming of minimally destructive DNA technologies—tools that might help us understand the lives of long-dead people without damaging their remains. I’m looking forward to covering those in the future. (In the meantime, I’m personally dreaming of a trip to—respectfully and carefully—visit Herculaneum.)
Now read the rest of The Checkup
Read more from MIT Technology Review‘s archive
Some believe an “ancient-DNA revolution” is underway, as scientists use modern technologies to learn about human, animal, and environmental remains from the past. My colleague Antonio Regalado has the details in his recent feature. The piece was published in the latest edition of our magazine, which focuses on relationships.
Next-generation obesity drugs might be too effective. One trial participant lost 22% of her body weight in nine months. Another lost 30% of his weight in just eight months. (STAT)
A US court upheld the conviction of Elizabeth Holmes, the disgraced founder of the biotechnology company Theranos, who was sentenced to over 11 years for defrauding investors out of hundreds of millions of dollars. Her sentence has since been reduced by two years for good behavior. (The Guardian)
An unvaccinated child died of measles in Texas. The death is the first reported as a result of the outbreak that is spreading in Texas and New Mexico, and the first measles death reported in the US in a decade. Health and Human Services Secretary Robert F. Kennedy Jr. appears to be downplaying the outbreak. (NBC News)
A mysterious disease with Ebola-like symptoms has emerged in the Democratic Republic of Congo. Hundreds of people have been infected in the last five weeks, and more than 50 people have died. (Wired)
Towana Looney has been discharged from the hospital three months after receiving a gene-edited pig kidney. “I’m so grateful to be alive and thankful to have received this incredible gift,” she said. (NYU Langone)
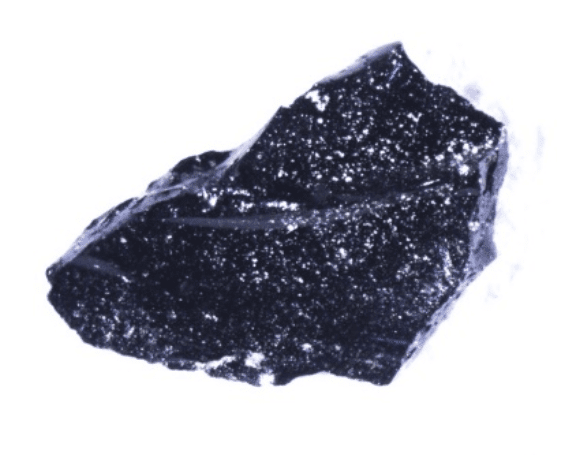
They look like small pieces of obsidian, smooth and shiny. But a set of small black fragments found inside the skull of a man who died in the eruption of Mount Vesuvius in Southern Italy, in the year 79 CE, are thought to be pieces of his brain—turned to glass.
The discovery, reported in 2020, was exciting because a human brain had never been found in this state. Now, scientists studying his remains believe they’ve found out more details about how the glass fragments were formed: The man was exposed to temperatures of over 500 °C, followed by rapid cooling. These conditions also allowed for the preservation of tiny structures and cells inside his brain.
“It’s an extraordinary finding,” says Matteo Borrini, a forensic anthropologist at Liverpool John Moores University in the UK, who was not involved in the research. “It tells us how [brain] preservation can work … extreme conditions can produce extreme results.”
Glittering remains
The Roman city of Herculaneum has been covered in ash for many hundreds of years. Excavations over the last few centuries have revealed amazing discoveries of preserved bodies, buildings, furniture, artworks, and even food. They’ve helped archaeologists piece together a picture of what life was like for people living in ancient Rome. But they are still yielding surprises.
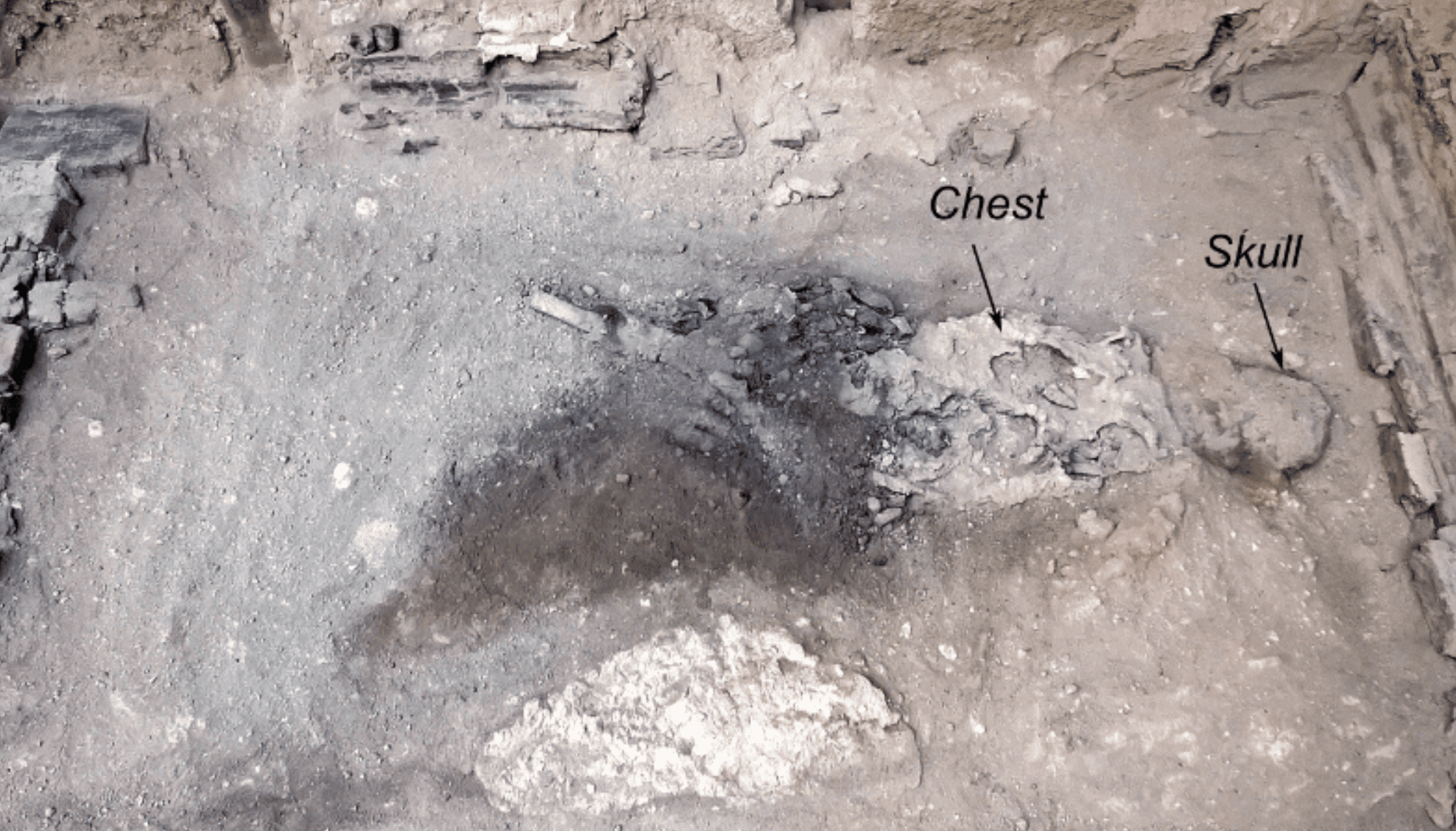
Around five years ago, Pier Paolo Petrone, a forensic archaeologist at the University of Naples Federico II, was studying remains first excavated in the 1960s of what is believed to be a 20-year-old man. The man was found inside a building thought to have been a place of worship. Archaeologists believe he may have been guarding the building. He was found lying face down on a wooden bed.
The carbonized remains of the deceased individual in their bed in Herculaneum.
GUIDO GIORDANO ET AL./SCIENTIFIC REPORTS
Petrone was documenting the man’s charred bones under a lamp when he noticed something unusual. “I suddenly saw small glassy remains glittering in the volcanic ash that filled the skull,” he tells MIT Technology Review via email. “It had a black appearance and shiny surfaces quite similar to obsidian.” But, he adds, “unlike obsidian, the glassy remains were extremely brittle and easy to crumble.”
An analysis of the proteins in the sample suggested that the glassy remains were preserved brain tissue. And when Petrone and his colleagues studied bits of the material with microscopes, they were even able to see neurons. “I [was] very excited because I understood that [the preserved brain] was something very unique, never seen before in any other archaeological or forensic context,” he says.
The next question was how the man’s brain turned to glass in the first place, says Guido Giordano, a volcanologist at Roma Tre University in Rome, who was also involved in the research. To find out, he and his colleagues subjected tiny pieces of the glass brain fragments—measuring millimeters wide—to extreme temperatures in the lab. The goal was to identify its “glass transition state”—the temperature at which the material changed from brittle to soft.
GUIDO GIORDANO ET AL./SCIENTIFIC REPORTS
These experiments suggest that the material is a glass, and that it formed when the temperature dropped from above 510 °C to room temperature, says Giordano. “The heating stage would not have been long. Otherwise the material would have been … cooked, and disappeared,” he says. This, he adds, is probably what happened to the brains of the other people whose remains were found at Herculaneum, which were not preserved.
The short periods of extremely high temperature might have resulted from super-hot volcanic gases and a few centimeters’ worth of ash, which enveloped the city shortly after the eruption and settled. Denser pyroclastic flows from the volcano would have hit the building hours later, possibly after the brain had a chance to rapidly cool down.
“The ash clouds can easily be 500 or 600 degrees … [but] they may quickly pass and quickly vanish,” says Giordano, who, along with his colleagues, published the results in the journal Scientific Reports on Thursday. “That would provide the fast cooling that is required to produce the glass.”
A unique case
No one knows for sure why this young man’s brain was the only one to form glass fragments. It might have been because he was sheltered inside the building, says Giordano. It is thought that most of Herculaneum’s other residents flocked to the city’s shores, hoping to be rescued.
It’s also not clear why the man was found lying face down on a bed. “We don’t know what he was doing,” says Giordano. He might not have been guarding the building at all, says Karl Harrison, a forensic archaeologist at the University of Exeter in the UK. “In a fire, people will end up in rooms they don’t know, because they’re running through smoke,” he says. The conditions may have been similar during the volcanic eruption. “People end up in funny places,” he adds.
Either way, it’s a unique finding. Archaeologists have unearthed ancient human brains before—over 4,400 have been discovered since the mid-17th century. But these samples tend to have been preserved through drying, freezing, or a process called saponification, in which the brains “effectively turn to soap,” says Harrison. He was involved in work on a site in Turkey at which an 8,000-year-old brain was found. That brain appears to have “carbonized” and turned charcoal-like, he says.
Some of the glassy brain fragments remain at the site in Herculaneum, but others are being kept at universities, where scientists plan to continue research on them. Petrone wants to further study the proteins in the samples to learn more about what’s in them.
Holding the fragments feels “quite amazing,” says Giordano. “A few times I stop and think: ‘I’m actually holding a bit of a brain of a human,’” he says. “It can be touching.”
This article first appeared in The Checkup, MIT Technology Review’s weekly biotech newsletter. To receive it in your inbox every Thursday, and read articles like this first, sign up here.
Yesterday marks a month since the inauguration of Donald Trump as the 47th US president. And what a month it has been. The Trump administration wasted no time in delivering a slew of executive orders, memos, and work notices to federal employees.
Making IVF more affordable and accessible should give people more options when it comes to family planning and reproductive freedom more generally. But the move comes after a barrage of actions by the new administration that are hitting reproductive care hard for people around the world. On January 20, his first day in office, Trump ordered a “90-day pause in United States foreign development assistance” for such programs to be assessed. By January 24, a “stop work” memo issued by the State Department brought US-funded aid programs around the world to a halt.
Recent estimates suggest that more than 8,000 women will die from complications related to pregnancy and childbirth over the next 90 days if the funding is not reinstated.
On January 24 Trump also reinstated the global gag rule—a policy that requires nongovernmental organizations receiving US health funding to agree that they will not offer abortion counseling and care. This move alone immediately stripped organizations of the funding they need to perform their work. MSI Reproductive Choices, which offers support for reproductive health care in 36 countries, lost $14 million as a result, says Anna Mackay, who manages donor-funded programs at the organization. “Over 2 million women and girls would have received contraceptive services with that money,” she says.
The US Agency for International Development (USAID) had a 2025 budget of $42.8 billion to spend on foreign assistance, which covers everything from humanitarian aid and sanitation to programs promoting gender equality and economic growth in countries around the world. But the “stop work” memo froze that funding for 90 days.
The impacts were felt immediately and are still rippling out. Clinical trials were halted. Jobs were lost. Health programs were shut down.
“I think this is going to have a devastating impact on the global health architecture,” says Thoai Ngo at Columbia University’s Mailman School of Public Health. “USAID is the major foreign funder for global health … I’m afraid that there isn’t [another government] that can fill the gap.”
Reproductive health care is likely to lose out as affected governments and health organizations try to reorganize their resources, says Ngo: “In times of crisis … women and girls tend to be deprioritized in terms of access to health and social services.”
Without information on and access to a range of contraceptive options, unintended pregnancies result. These have the potential to limit the freedoms of people who become pregnant. And they can have far-reaching economic impacts, since access to contraception can improve education rates and career outcomes.
And the health consequences can be devastating. Unintended pregnancies are more likely to be ended with abortions—potentially unsafe ones. Maternal death rates are high in regions that lack adequate resources. A maternal death occurred every two minutes in 2020.
“It’s difficult to overstate how catastrophic this freeze has been over the last several weeks,” says Amy Friedrich-Karnik, director of federal policy at the Guttmacher Institute, a research and policy organization focused on global sexual and reproductive health and rights. “Every single day that the freeze is in place, there are 130,000 women who are being denied contraceptive care,” she says.
The Guttmacher Institute estimates that should USAID funding be frozen for the full 90 days, around 11.7 million women and girls would lose access to contraceptive care, and 4.2 million of them would experience unintended pregnancies. Of those, “8,340 will die from complications during pregnancy and childbirth,” says Friedrich-Karnik.
“By denying people access to contraception, not only are you denying them tools for their bodily autonomy—you are really risking their lives,” she says. “Thousands more women will die down the road.”
“USAID plays such a central role in supporting these life-saving programs,” says Ngo. “The picture is bleak.”
Even online sources of information on contraceptives are being affected by the funding freeze. Ben Bellows is a chief business officer at Nivi, a digital health company that develops chatbots to deliver health information to people via WhatsApp. “Two million users have used the bot,” he says.
He and his team have been working on a project to deliver information on contraceptive options and family planning to women in India, and they have been looking to incorporate AI into their bot. The project was funded by a company that, in turn, is funded by USAID. Like the funding, the work is “frozen,” says Bellows.
“We’ve slowed [hiring] and we’ve slowed some of the tech development because of the freeze [on USAID],” he says. “It’s bad [for] the individuals, it’s bad [for] the companies that are trying to operate in these markets, and it’s bad [for] public health outcomes.”
Reproductive health and freedoms are also likely to be affected by the Trump administration’s cuts to federal agencies. The National Institutes of Health and the Centers for Disease Control and Prevention have been in the administration’s crosshairs, as has the Food and Drug Administration.
After all, the FDA regulates drugs and medical devices in the US, including contraceptives. The CDC collects and shares important data on sexual and reproductive health. And the NIH supports vital research on reproductive health and contraception.
The CDC also funds health programs in low-income countries like Ethiopia. Following Trump’s executive order, the country’s ministry of health terminated the contracts of more than 5,000 health workers whose salaries were supported by the CDC as well as USAID.
“That’s midwives and nurses working in rural health posts,” says Mackay. “We’re turning up to support these staff and provide them with sexual reproductive health training and make sure they’ve got the contraceptives, and there’s just no one at the facility.”
So, yes, it is great news if the Trump administration can find a way to make IVF more accessible. But, as Mackay points out, “it’s increasing reproductive choice in one direction.”
My colleague Rhiannon Williams reported on the immediate aftermath of the decision that reversed Roe v. Wade.
Fertility rates are falling around the world, in almost every country. IVF is great, but it won’t save us from a looming fertility crisis. Gender equality and family-friendly policies are much more likely to be effective.
Decades of increasingly successful IVF treatments have caused millions of embryos to be stored in cryopreservation tanks around the world. In some cases, they can’t be donated, used, or destroyed and appear to be stuck in limbo “forever.”
Ever come across the term “women of childbearing age”? The insidious idea that women’s bodies are, above all else, vessels for growing children has plenty of negative consequences for us all. But it has also set back scientific research and health policy.
The US Food and Drug Administration assesses the efficacy and toxicity of experimental medicines before they are approved. It should also consider their “financial toxicity,” given that medical bills can fall on the shoulders of patients themselves, argue a group of US doctors. (The New England Journal of Medicine)
Robert F. Kennedy Jr., the new US secretary of health and human services, has vowed to investigate the country’s childhood vaccination schedule. During his confirmation hearing a couple of weeks ago, he promised not to change the schedule. (Associated Press)
Some scientists have been altering their published work without telling anyone. Such “stealth corrections” threaten scientific integrity, say a group of researchers from Europe and the US. (Learned Publishing)
The US Department of Agriculture said it accidentally fired several people who were working on the federal response to the bird flu outbreak. Apparently the agency is now trying to hire them back. (NBC News)
Could your next pet be a glowing rabbit? This startup is using CRISPR to “level up” pets. Their goal is to eventually create a real-life unicorn. (Wired)
Eske Willerslev was on a tour of Montreal’s Redpath Museum, a Victorian-era natural history collection of 700,000 objects, many displayed in wood and glass cabinets. The collection—“very, very eclectic,” a curator explained—reflects the taste in souvenirs of 19th-century travelers and geology buffs. A visitor can see a leg bone from an extinct Steller’s sea cow, a suit of samurai armor, a stuffed cougar, and two human mummies.
Willerslev, a well-known specialist in obtaining DNA from old bones and objects, saw potential biological samples throughout this hodgepodge of artifacts. Glancing at a small Egyptian cooking pot, he asked the tour leader, “Do you ever find any grain in these?” After studying a dinosaur skeleton that proved to be a cast, not actual bone, he said: “Too bad. There can be proteins on the teeth.”
“I am always thinking, ‘Is there something interesting to take DNA from?’” he said, glancing at the curators. “But they don’t like it, because …” Willerslev, who until recently traveled with a small power saw, made a back-and-forth slicing motion with his hand.
Willerslev was visiting Montreal to receive a science prize from the World Cultural Council—one previously given to the string theorist Edward Witten and the astrophysicist Margaret Burbidge, for her work on quasars. Willerslev won it for “numerous breakthroughs in evolutionary genetics.” These include recovering the first more or less complete genome of an ancient man, in 2010, and setting a record for the oldest genetic material ever retrieved: 2.4-million-year-old genes from a frozen mound in Greenland, which revealed that the Arctic desert was once a forest, complete with poplar, birch, and roaming mastodons.
These findings are only part of a wave of discoveries from what’s being called an “ancient-DNA revolution,” in which the same high-speed equipment used to study the DNA of living things is being turned on specimens from the past. At the Globe Institute, part of the University of Copenhagen, where Willerslev works, there’s a freezer full of human molars and ear bones cut from skeletons previously unearthed by archaeologists. Another holds sediment cores drilled from lake bottoms, in which his group is finding traces of entire ecosystems that no longer exist.
“We’re literally walking on DNA, both from the present and from the past.”
Eske Willerslev
Thanks to a few well-funded labs like the one in Copenhagen, the gene time machine has never been so busy. There are genetic maps of saber-toothed cats, cave bears, and thousands of ancient humans, including Vikings, Polynesian navigators, and numerous Neanderthals. The total number of ancient humans studied is more than 10,000 and rising fast, according to a December 2024 tally that appeared in Nature. The sources of DNA are increasing too. Researchers managed to retrieve an Ice Age woman’s genome from a carved reindeer tooth, whose surface had absorbed her DNA. Others are digging at cave floors and coming up with records of people and animals that lived there.
“We’re literally walking on DNA, both from the present and from the past,” Willerslev says.
Eske Willerslev leads one of a handful of laboratories pioneering the extraction and sequencing of ancient DNA from humans, animals, and the environment. His group’s main competition is at Harvard University and at the Max Planck Institute for Evolutionary Anthropology in Leipzig, Germany.
JONAS PRYNER ANDERSEN
The old genes have already revealed remarkable stories of human migrations around the globe. But researchers are hoping ancient DNA will be more than a telescope on the past—they hope it will have concrete practical use in the present. Some have already started mining the DNA of our ancestors for clues to the origin of modern diseases, like diabetes and autoimmune conditions. Others aspire to use the old genetic data to modify organisms that exist today.
At Willerslev’s center, for example, a grant of 500 million kroner ($69 million) from the foundation that owns the Danish drug company Novo Nordisk is underwriting a project whose aims include incorporating DNA variation from plants that lived in ancient climates into the genomes of food crops like barley, wheat, and rice. The plan is to redesign crops and even entire ecosystems to resist rising temperatures or unpredictable weather, and it is already underway—last year, barley shoots bearing genetic information from plants that lived in Greenland 2 million years ago, when temperatures there were far higher than today, started springing up in experimental greenhouses.
Willerslev, who started out looking for genetic material in ice cores, is leaning into this possibility as the next frontier of ancient-DNA research, a way to turn it from historical curiosity to potential planet-saver. If nothing is done to help food crops adapt to climate change, “people will starve,” he says. “But if we go back into the past in different climate regimes around the world, then we should be able to find genetic adaptations that are useful. It’s nature’s own response to a climate event. And can we get that? Yes, I believe we can.”
Shreds and traces
In 1993, just a day before the release of the blockbuster Steven Spielberg film Jurassic Park, scientists claimed in a paper that they had extracted DNA from a 120-million-year-old weevil preserved in amber. The discovery seemed to bring the film’s premise of a cloned T. rex closer to reality. “Sooner or later,” a scientist said at the time, “we’re going to find amber containing some biting insect that filled its stomach with blood from a dinosaur.”
But those results turned out to be false—likely the result of contamination by modern DNA. The problem is that modern DNA is much more abundant than what’s left in an old tooth or sample of dirt. That’s because the genetic molecule is constantly chomped on by microbes and broken up by water and radiation. Over time, the fragments get smaller and smaller, until most are so short that no one can tell whether they belonged to a person or a saber-toothed cat.
“Imagine an ancient genome as a big old book, and that all the pages have been torn out, put through a shredder, and tossed into the air to be lost with the wind. Only a few shreds of paper remain. Even worse, they are mixed with shreds of paper from other books, old and new,” says Elizabeth Jones, a science historian. Her 2022 book, Ancient DNA: The Making of a Celebrity Science, details researchers’ overwhelming fear of contamination—both literal, from modern DNA, and of the more figurative sort that can occur when scientists are so tempted by the prospect of fame and being first that they risk spinning sparse data into far-fetched stories.
“When I entered the field, my supervisor said this is a very, very dodgy path to take,” says Willerslev.
But the problem of mixed-up and fragmented old genes was largely solved beginning in 2005, when US companies first introduced ultra-fast next-generation machinery for analyzing genomes. These machines, meant for medical research, required short fragments for fast performance. And ancient-DNA researchers found they could use them to brute-force their way through even poorly preserved samples. Almost immediately, they started recovering large parts of the genomes of cave bears and woolly mammoths.
Ancient humans were not far behind. Willerslev, who was not yet famous, didn’t have access to human bones, and definitely not the bones of Neanderthals (the best ones had been corralled by the scientist Svante Pääbo, who was already analyzing them with next-gen sequencers in Germany). But Willerslev did learn about a six-inch-long tuft of hair collected from a 4,000-year-old midden, or trash heap, on Greenland’s coast. The hair had been stored in a plastic bag in Denmark’s National Museum for years. When he asked about it, curators told him they thought it was human but couldn’t be sure.
“Well, I mean, do you know any other animal in Greenland with straight black hair?” he says. “Not really, right?”
The hair turned out to contain well-preserved DNA, and in 2010, Willerslev published a paper in Nature describing the genome of “an extinct Paleo-Eskimo.” It was the first more or less complete human genome from the deep past. What it showed was a man with type A+ blood, probably brown eyes and thick dark hair, and—most tellingly—no descendants. His DNA code had unique patterns not found in the Inuit who occupy Greenland today.
“Give the archaeologists credit … because they have the hypothesis. But we can nail it and say, ‘Yes, this is what happened.’”
Lasse Vinner
The hair had come from a site once occupied by a group called the Saqqaq, who first reached Greenland around 4,500 years ago. Archaeologists already knew that the Saqqaq’s particular style of making bird darts and spears had vanished suddenly, but perhaps that was because they’d merged with another group or moved away. Now the man’s genome, with specific features pointing to a genetic dead end, suggested they really had died out, very possibly because extreme isolation, and inbreeding, had left them vulnerable. Maybe there was a bad year when the migrating reindeer did not appear.
“Give the archaeologists credit … because they have the hypothesis. But we can nail it and say, ‘Yes, this is what happened,’” says Lasse Vinner, who oversees daily operations at the Copenhagen ancient-DNA lab. “We’ve substantiated or falsified a number of archaeological hypotheses.”
In November, Vinner, zipped into head-to-toe white coveralls, led a tour through the Copenhagen labs, located in the basement of the city’s Natural History Museum. Samples are processed there in a series of cleanrooms under positive air pressure. In one, the floors were still wet with bleach—just one of the elaborate measures taken to prevent modern DNA from getting in, whether from a researcher’s shoes or from floating pollen. It’s partly because of the costly technologies, cleanrooms, and analytical expertise required for the work that research on ancient human DNA is dominated by a few powerful labs—in Copenhagen, at Harvard University, and in Leipzig, Germany—that engage in fierce competition for valuable samples and discoveries. A 2019 New York Times Magazine investigation described the field as an “oligopoly,” rife with perverse incentives and a smash-and-grab culture—in other words, artifact chasing straight out of Raiders of the Lost Ark.
To get his share, Willerslev has relied on his growing celebrity, projecting the image of a modern-day explorer who is always ready to trade his tweeds for muck boots and venture to some frozen landscape or Native American cave. Add to that a tale of redemption. Willerslev often recounts his struggles in school and as a would-be mink hunter in Siberia (“I’m not only a bad student—I’m also a tremendously bad trapper,” he says) before his luck changed once he found science.
This narrative has made him a favorite on television programs like Nova and secured lavish funding from Danish corporations. His first autobiography was titled From Fur Hunter to Professor. A more recent one is called simply It’s a Fucking Adventure.
Peering into the past
The scramble for old bones has produced a parade of headlines about the peopling of the planet, and especially of western Eurasia—from Iceland to Tehran, roughly. That’s where most ancient DNA samples originate, thanks to colder weather, centuries of archaeology, and active research programs. At the National Museum in Copenhagen, some skeletons on display to the public have missing teeth—teeth that ended up in the Globe Institute’s ancient-DNA lab as part of a project to analyze 5,000 sets of remains from Eurasia, touted as the largest single trove of old genomes yet.
What ancient DNA uncovered in Europe is a broad-brush story of three population waves of modern humans. First to come out of Africa were hunter-gatherers who dispersed around the continent, followed by farmers who spread out of Anatolia starting 11,000 years ago. That wave saw the establishment of agriculture and ceramics and brought new stone tools. Last came a sweeping incursion of people (and genes) from the plains of modern Ukraine and Russia—animal herders known as the Yamnaya, who surged into Western Europe spreading the roots of the Indo-European languages now spoken from Dublin to Bombay.
Mixed history
The DNA in ancient human skeletons reveals prehistoric migrations.
The genetic background of Europeans was shaped by three major migrations starting about 45,000 years ago. First came hunter-gatherers. Next came farmers from Anatolia, bringing crops and new ways of living. Lastly, mobile herders called the Yamnaya spread from the steppes of modern Russia and Ukraine. The DNA in ancient skeletons holds a record of these dramatic population changes.
Adapted from “100 ancient genomes show repeated population turnovers in Neolithic Denmark,” Nature, January 10, 2024, and “Tracing the peopling of the world through genomics,” Nature, January 18, 2017
Archaeologists had already pieced together an outline of this history through material culture, examining shifts in pottery styles and burial methods, the switch from stone axes to metal ones. Some attributed those changes to cultural transmission of knowledge rather than population movements, a view encapsulated in the phrase “pots, not people.” However, ancient DNA showed that much of the change was, in fact, the result of large-scale migration, not all of which looks peaceful. Indeed, in Denmark, the hunter-gatherer DNA signature all but vanishes within just two generations after the arrival of farmers during the late Stone Age. To Willerslev, the rapid population replacement “looks like some kind of genocide, to be honest.” It’s a guess, of course, but how else to explain the “limited genetic contribution” to subsequent generations of the blue-eyed, dark-haired locals who’d fished and hunted around Denmark’s islands for nearly 5,000 years? Certainly, the bodies in Copenhagen’s museums suggest violence—some have head injuries, and one still has arrows in it.
In other cases, it’s obvious that populations met and mixed; the average ethnic European today shares some genetic contribution from all three founding groups—hunter, farmer, and herder—and a little bit from Neanderthals, too.“We had the idea that people stay put, and if things change, it’s because people learned to do something new, through movements of ideas,” says Willerslev. “Ancient DNA showed that is not the case—that the transitions from hunter-gatherers to farming, from bronze to iron, from iron to Viking, [are] actually due to people coming and going, mixing up and bringing new knowledge.” It means the world that we observe today, with Poles in Poland and Greeks in Greece, “is very, very young.”
With an increasing number of old bodies giving up their DNA secrets, researchers have started to search for evidence of genetic adaptation that has occurred in humans since the last ice age (which ended about 12,000 years ago), a period that the Copenhagen group noted, in a January 2024 report, “involved some of the most dramatic changes in diet, health, and social organization experienced during recent human evolution.”
Every human gene typically comes in a few different possible versions, and by studying old bodies, it’s possible to see which of these versions became more common or less so with time—potentially an indicator that they’re “under selection,” meaning they influenced the odds that a person stayed alive to reproduce. These pressures are often closely tied to the environment. One clear signal that pops out of ancient European genes is a trend toward lighter skin—which makes it easier to produce vitamin D in the face of diminished sunlight and a diet based on grains.
DNA from ancient human skeletons could help us understand the origins of modern diseases, like multiple sclerosis.
MIKAL SCHLOSSER/UNIVERSITY OF COPENHAGEN
New technology and changing lifestyles—like agriculture and living in proximity to herd animals (and their diseases)—were also potent forces. Last fall, when Harvard University scientists scanned DNA from skeletons, they said they’d detected “rampant” evidence of evolutionary action. The shifts appeared especially in immune system genes and in a definite trend toward less body fat, the genetic markers of which they found had decreased significantly “over ten millennia.” That finding, they said, was consistent with the “thrifty gene” hypothesis, a feast-or-famine theory developed in the 1960s, which states that before the development of farming, people needed to store up more food energy, but doing so became less of an advantage as food became more abundant.
Many of the same genes that put people at risk for multiple sclerosis today almost certainly had some benefit in the past.
Such discoveries could start to explain some modern disease mysteries, such as why multiple sclerosis is unusually common in Nordic countries, a pattern that has perplexed doctors.
The condition seems to be a “latitudinal disease,” becoming more prevalent the farther north you go; theories have pointed to factors including the relative lack of sunlight. In January of last year, the Copenhagen team, along with colleagues, claimed that ancient DNA had solved the riddle, saying the increased risk could be explained in part by the very high amount of Yamnaya ancestry among people in Sweden, Norway, and Denmark.
When they looked at modern people, they found that mutations known to increase the risk of multiple sclerosis were far more likely to occur in stretches of DNA people had inherited from these Yamnaya ancestors than in parts of their genomes originating elsewhere.
There’s a twist to the story: Many of the same genes that put people at risk for multiple sclerosis today almost certainly had some benefit in the past. In fact, there’s a clear signal these gene versions were once strongly favored and on the increase. Will Barrie, a postdoc at Cambridge University who collaborated on the research, says the benefit could have been related to germs and infections that these pastoralists were getting from animals. But if modern people don’t face the same exposures, their immune system might still try to box at shadows, resulting in autoimmune disease. That aligns with evidence that children who aren’t exposed to enough pathogens may be more likely to develop allergies and other problems later in life.
“I think the whole sort of lesson of this work is, like, we are living with immune systems that we have inherited from our past,” says Barrie. “And we’ve plunged it into a completely new, modern environment, which is often, you know, sanitary.”
Telling stories about human evolution often involves substantial guesswork—findings are frequently reversed. But the researchers in Copenhagen say they will be trying to more systematically scan the past for health clues. In addition to the DNA of ancient peoples, they’re adding genetic information on what pathogens these people were infected with (germs based on DNA, like plague bacteria, can also get picked up by the sequencers), as well as environmental data, such as average temperatures at points in the past, or the amount of tree cover, which can give an idea of how much animal herding was going on. The resulting “panels”—of people, pathogens, and environments—could help scientists reach stronger conclusions about cause and effect.
Some see in this research the promise of a new kind of “evolutionary medicine”—drugs tailored to your ancestry. However, the research is not far enough along to propose a solution for multiple sclerosis.
For now, it’s just interesting. Barrie says several multiple sclerosis patients have written him and said they were comforted to think their affliction had an explanation. “We know that [the genetic variants] were helpful in the past. They’re there for a reason, a good reason—they really did help your ancestors survive,” he says. “I hope that’s helpful to people in some sense.”
Bringing things back
In Jurassic Park, which was the highest-grossing movie of all time until Titanic came out in 1997, scientists don’t just get hold of old DNA. They also use it to bring dinosaurs back to life, a development that leads to action-packed and deadly consequences.
The idea seemed like fantasy when the film debuted. But Jurassic Park presaged current ambitions to bring past genes into the present. Some of these efforts are small in scale. In 2021, for instance, researchers added a Neanderthal gene to human cells and turned those into brain organoids, which they reported were smaller and lumpier than expected. Others are aiming for living animals. Texas-based Colossal Biosciences, which calls itself the “first de-extinction company,” says it will be trying to use a combination of gene editing, cloning, and artificial wombs to re-create extinct species such as mammoths and the Tasmanian tiger, or thylacine.
Colossal recently recruited a well-known paleogenomics expert, Beth Shapiro, to be its chief scientist. In 2022, Shapiro, previously an advisor to the company, said that she had sequenced the genome of an extinct dodo bird from a skull kept in a museum. “The past, by its nature, is different from anything that exists today,” says Shapiro, explaining that Colossal is “reaching into the past to discover evolutionary innovations that we might use to help species and ecosystems thrive today and into the future.”
The idea of bringing extinct animals back to life seemed like fantasy when Jurassic Park debuted. But the film presaged current ambitions to bring past genes into the present.
It’s not yet clear how realistic the company’s plan to reintroduce missing species and restore nature’s balance really is, although the public would likely buy tickets to see even a poor copy of an extinct animal. Some similar practical questions surround the large grant Willerslev won last year from the philanthropic foundation of Novo Nordisk, whose anti-obesity drugs have turned it into Denmark’s most valuable company.
The project’s concept is to read the blueprints of long-gone ecosystems and look for genetic information that might help major food crops succeed in shorter or hotter growing seasons. Willerslev says he’s concerned that climate change will be unpredictable—it’s hard to say if it will be too wet in any particular area or too dry. But the past could offer a data bank of plausible solutions, which he thinks needs to be prepared now.
The prototype project is already underway using unusual mutations in plant DNA found in the 2-million-year-old dirt samples from Greenland. Some of these have been introduced into modern barley plants by the Carlsberg Group, a brewer that is among the world’s largest beer companies and operates an extensive crop lab in Copenhagen.
Eske Willerslev collects samples in the Canadian Arctic during a summer 2024 field trip. DNA preserved in soil could help determine how megafauna, like the woolly mammoth, went extinct.
RYAN WILKES/UNIVERSITY OF COPENHAGEN
One gene being studied is for a blue-light receptor, a protein that helps plants decide when to flower—a trait also of interest to modern breeders. Two and a half million years ago, the world was warm, and parts of Greenland particularly so—more than 10 °C hotter than today. That is why vegetation could grow there. But Greenland hasn’t moved, so the plants must have also been specially adapted to the stress of a months-long dusk followed by weeks of 24-hour sunlight. Willerslev says barley plants with the mutation are already being grown under different artificial light conditions, to see the effects.
“Our hypothesis is that you could use ancient DNA to identify new traits and as a blueprint for modern crop breeding,” says Birgitte Skadhauge, who leads the Carlsberg Research Laboratory. The immediate question is whether barley can grow in the high north—say, in Greenland or upper Norway, something that could be important on a warming planet. The research is considered exploratory and separate from Carlsberg’s usual commercial efforts to discover useful traits that cut costs—of interest since it brews 10 billion liters of beer a year, or enough to fill the Empire State Building nine times.
Scientists often try hit-or-miss strategies to change plant traits. But Skadhauge says plants from unusual environments, like a warm Greenland during the Pleistocene era, will have incorporated the DNA changes that are important already. “Nature, you know, actually adapted the plants,” she says. “It already picked the mutation that was useful to it. And if nature has adapted to climate change over so many thousands of years, why not reuse some of that genetic information?”
Many of the lake cores being tapped by the Copenhagen researchers cover more recent times, only 3,000 to 10,000 years ago. But the researchers can also use those to search for ideas—say, by tracing the genetic changes humans imposed on barley as they bred it to become one of humanity’s “founder crops.” Among the earliest changes people chose were those leading to “naked” seeds, since seeds with a sticky husk, while good for making beer, tend to be less edible. Skadhauge says the team may be able to reconstruct barley’s domestication, step by step.
There isn’t much precedent for causing genetic information to time-travel forward. To avoid any Jurassic Park–type mishaps, Willerslev says, he’s building a substantial ethics team “for dealing with questions about what does it mean if you’re introducing ancient traits into the world.” The team will have to think about the possibility that those plants could outcompete today’s varieties, or that the benefits would be unevenly distributed—helping northern countries, for example, and not those closer to the equator.
Willerslev says his lab’s evolution away from human bones toward much older DNA is intentional. He strongly hints that the team has already beat its own record for the oldest genes, going back even more than 2.4 million years. And as the first to look further back in time, he’s certain to make big discoveries—and more headlines. “It’s a blue ocean,” he says—one that no one has ever seen.
A new adventure, he says, is practically guaranteed.